
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Transitional cell carcinoma of the bladder with hepatoid differentiation: A case report
Selim Tas; Ali Erhan Eren*
Antalya Provincal Health Directorate, Antalya Training and Research Hospital, Turkey.
*Corresponding Author : Ali Erhan Eren
Department of Urology, Antalya Education and Research Hospital, University of Health Sciences, Varlık
Mahallesi, Kazim Karabekir Caddesi, 07100, Muratpasa, Antalya-Turkey.
Email: erenalierhan@yahoo.com
Received : Feb 25, 2021
Accepted : Apr 02, 2021
Published : Apr 06, 2021
Archived : www.jcimcr.org
Copyright : © Eren AE (2021).
Citation: Tas T, Eren AE. Transitional cell carcinoma of the bladder with hepatoid differentiation: A case report. J Clin Images Med Case Rep. 2021; 2(2): 1042.
Introduction
Hepatoid adenocarcinoma is a very rare disease and usually occurs in the stomach, ovaries and lungs. The term hepatoid adenocarcinoma was first introduced by Ishikura et al. in 1985 to describe a rare aggressive malignant neoplasm in the urinary bladder [1,3].
Case presentation
A 59-year-old male patient with hematuria was admitted to our emergency department with the complaint of deterioration of the general condition. The complete blood count detected a hemoglobin level of 4 mg/dl. 4vünites erythrocyte suspensions were transfused. The medical history showed complaints of hematuria for the last 6 months. Computed tomography imaging study showed multiple millimetric masses in the liver that completely filled the bladder.
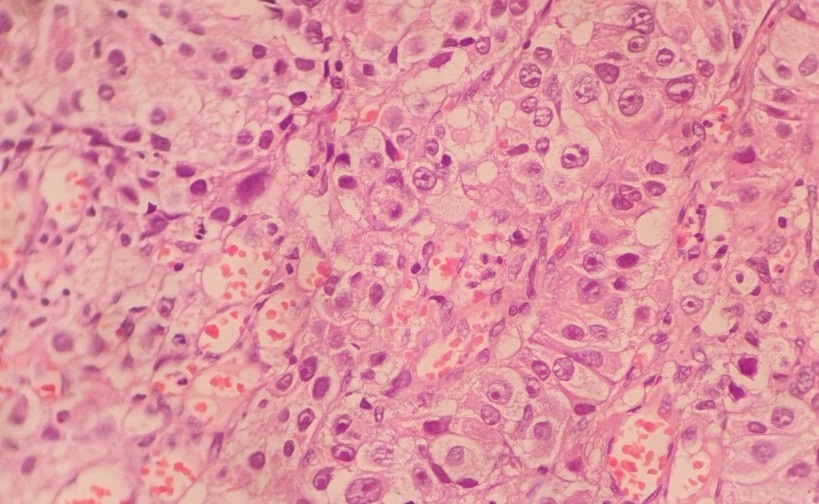
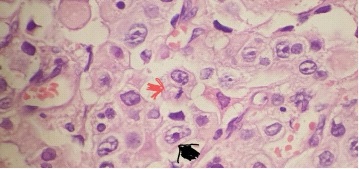
The patient was scheduled for cystoscopic examination. Cystoscopic examination revealed a tumor that completely filled the inside of the bladder. Subsequently, incomplete Transurethral Resection of Bladder Tumor (TURBT) was performed. Pathological examination resulted in HAC invading muscle. Tumor cells were microscopically typed as a hepatocellular carcinoma containing large and polygonal cells with marked nuclear atypia and eosinophilic granular or clear cytoplasm.
Serum concentration of AFP was within normal limits. Liver function test results were within the normal reference range. The levels of serological markers for HBV and HCV were also within normal limits. In the staging study, thoracic CT imaging showed normal pulmonary structures, but hepatic USG examination showed multiple metastatic lesions with millimetric sizes and isoechoic and heterogeneous structures. On the second postoperative day, a thrombosis was detected in the right iliac vein. The patient was scheduled for chemotherapy and concurrent radiotherapy died at 2 months of follow-up.

Discussion
In the literature, the term "Hepatoid" has been used to denote a heterogeneous type of tumor in various organs [3-9] which can be subdivided into three broad categories. Hepatoid adenocarcinomas are extrahepatic tumors that have areas morphologically comparable with hepatocellular carcinomas [10, 11].
Metzgeroth et al. published a review of 262 patients with HAC. Gastric involvement had the highest rate with 63%. Stomach (63%) had the highest rate of involvement, followed by ovaries (10%), lungs (4%), gall bladder (3%), pancreas (4%), uterus (4%) and urinary bladder (3%). HAC usually occurs in elderly patients. The male/female ratio was 2.4/1 and the median age at diagnosis was 65 years [12].
From a clinical point of view, it may be appropriate for pathologists to assist clinicians in establishing the correct diagnosis of primary hepatoid adenocarcinoma and thus ensuring appropriate management of patients [8,13,14]. It has been shown that carcinomas with hepatoid features, regardless of AFP production, have a worse prognosis than AFP-producing carcinomas without hepatoid morphological features [6].
In a case report on 4 patients, A. Lopez-Beltran et al. showed that a low pathological stage of the tumor (pT1) may be associated with longer survival times [15]. Ishikura H.et al. HAC case (stage I) in renal pelvis has seen similiar findings. It was treated with a local excision procedure [6]. In a case report, SekinoY. et al. performed transurethral resection and detected HAC (pT1) in the urinary bladder. Moreover, they did not detect any recurrence during the 20-month follow-up [2].
As seen in our case, normal serum levels of AFP and a muscle-invasive HAC (pT2) have negative effects on survival times. Hepatoid adenocarcinoma is a highly aggressive tumor that mimics the histological appearance of hepatocellular carcinoma. Current data show a close relationship between the pathological stage at diagnosis and survival times.
Conclusion
HAC is a highly aggressive tumor that mimics the histological appearance of hepatocellular carcinoma. AFP-producing HACs have a more aggressive course than non-AFP-producing HACs. There are very few published reports reporting HAC in the urinary bladder. It is important to be aware of atypical localizations of cancers in order to establish an accurate diagnosis.
Patient consent
Written informed consent was obtained from patient before surgery, and our study was conducted according to the permission of patient
References
- Erdemir F, Tunc M, Özcan F ve et al. The effect of squamous and/ or glandular differentiation on recurrence, progression and survival in urothelial carcinoma of bladder. Int Urol Nephrol. 2007; 39: 803-807.
- Sekino Y, Mochizuki H and Kuniyasu H. A 49-year-old woman presenting with hepatoid adenocarcinoma of the urinary bladder: A case report. Journal of Medical Case Reports. 2013; 7: 12.
- Ishikura H, Scully RF. Hepatoid carcinoma of the ovary. A newly described tumor. Cancer. 1987; 60: 2775–2784.
- Shikura H, Fukasawa Y, Ogasawara K, Natori T, Tsukuda Y, Aizawa M. An AFP-producing gastric carcinoma with features of hepatic differentiation: A case report. Cancer. 1985; 56: 840–848.
- Ishikura H, Kirimoto K, Sakamoto M, Miyamoto Y, Yamagiwa H, Troh T, et al. Hepatoid adenocarcinoma of the stomach: an analysis of seven cases. Cancer. 1986; 58: 119–126.
- Ishikura H, Ishiguro T, Eantus C, et al. Hepatoid adenocarcinoma of the renal pelvis producing alpha-fetoprotein of hepatic type and bile pigment. Cancer. 1991; 67: 3051–3056.
- Nogales EF, Concha A, Plata C, Ruiz-Avila I. Granulosa cell tumor of the ovary with diffuse true hepatic differentiation simulating stromal luteinization. Am J Surg Pathol. 1993; 17: 85–90.
- Sinard J, Macleary L Jr. Melamed J. Hepatoid adenocarcinoma of the urinary bladder. Unusual localization or a newly recognized tumor type. Cancer. 1994; 73: 1919–1925.
- Yamamoto R, Ishikura H, Azuma M, Hareyama H, Makinoda S, Koyama Y, et al. Alpha-fetoprotein production by a hepatoid adenocarcinoma of the uterus. J Clin Pathol. 1996; 49: 420–422.
- Arnould L, Drouer P, Fargeot P, Bernard A, Foucher P, Collin E, et al. Hepatoid adenocarcinoma of the lung: Report of a case of an unusual alpha-fetoprotein-producing lung tumor. Am J Surg Pathol. 1997; 21: 1113–1118.
- Bostwick DG, Lopez-Beltran A. Bladder Biopsy Interpretation. United Pathologists Press, New York. 1999; 173–196.
- Metzgeroth G, Strobel P, Baumbusch T, Reiter A, Hastka J. Hepatoid adenocarcinoma - review of the literature illustrated by a rare case originating in the peritoneal cavity Onkologie. 2010; 33: 263-269.
- Burgues O, Ferrer J, Navarro S, Ramos D, Botella E, LlombartBosch A. Hepatoid adenocarcinoma of the urinary bladder. An unusual neoplasm. Virchows Arch. 1999; 435: 71–75.
- Yamada K, Fujioka Y, Ebihara Y, Kiriyama I, Suzuki H, Akimoto M. Alpha-fetoprotein producing undifferentiated carcinoma of the bladder. J Urol 1994; 152: 958–960.
- Lopez-Beltran, RJ Luque, A. Quintero, MJ Requena, R. Montironi, blader hepatoid adenokarsinomu, Virchows Archiv. 10.1007 / s00428-003-0772-8. 2003; 442: 381-387.