
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Thyroglossal duct cyst presenting as life-threatening airway obstruction in a neonate
Duha Hejla1; Erella Elkon-Tamir1; Li-tal Pratt2 ; Oshri Wasserzug3,4; Leonor Leider-Trejo5; Avivit Brener1; Yael Lebenthal1*
1 Pediatric Endocrinology and Diabetes Unit, Dana-Dwek Children’s Hospital, Israel.
2 Pediatric Radiology Unit, Dana-Dwek Children’s Hospital, Israel.
3 Pediatric ENT Unit, Dana-Dwek Children’s Hospital, Israel.
4 Department of Otolaryngology, Head & Neck and Maxillofacial Surgery, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel
5 Institute of Pathology, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel.
*Corresponding Author : Yael Lebenthal
Pediatric Endocrinology and Diabetes Unit, Dana Dwek
Children’s Hospital, Tel Aviv Sourasky Medical Center, 6
Weizmann Street, Tel Aviv 64239-06, Israel.
Email: yaelleb@tlvmc.gov.il
Received : Feb 08, 2021
Accepted : Apr 13, 2021
Published : Apr 15, 2021
Archived : www.jcimcr.org
Copyright : © Lebenthal Y (2021).
Keywords: Thyroglossal duct cyst; Neonate; Airway compromise; Ectopic thyroid tissue; hypothyroidism.
Citation: Hejla D, Elkon-Tamir E, Pratt L, Wasserzug O, Leider-Trejo L. Thyroglossal duct cyst presenting as life-threatening airway obstruction in a neonate. J Clin Images Med Case Rep. 2021; 2(2): 1049.
Case report
Thyroglossal duct cysts are the most common congenital abnormality in the neck, accounting for 70-75% of midline neck masses in children [1]. Late in the 4th week of gestation, the thyroid anlage develops as a small, solid mass of endoderm proliferating at the foramen cecum. As the thyroid anlage descends caudally in the neck, it maintains an attachment to the site of origin at the level of the foramen cecum of the tongue via the thyroglossal duct [2]. The thyroglossal duct typically involutes and atrophies between 7 and 10 weeks of gestation by the time the thyroid gland reaches its final position inferior to the cricoid cartilage [2]. The source of TGDC is believed to be persistent remnants of the thyroglossal duct. Due to the communication of the duct to the mouth via the foramen cecum, thyroglossal cysts can become infected with oral flora. One-third of patients of all ages will present with a concurrent or prior infection, and one-quarter will present with a draining sinus from spontaneous or incisional drainage of an abscess [3]. The cysts occur almost equally in both sexes [4,5].
Patient description
A 9-day-old male presented to the pediatric emergency department with intermittent cyanosis, eating difficulties, and weight loss with no apparent evidence of fever, upper respiratory tract infection, or convulsions. The routine pregnancy monitoring had been unremarkable, including first trimester triple screen test, nuchal translucency, and a comprehensive detailed evaluation of the fetal anatomy ultrasound (US) in the second trimester. He was delivered via C-section due to breech presentation at 39 weeks’ gestation with a birth weight of 3,115 grams (appropriate for gestational age).
On admission to the emergency department, he appeared alert and free of distress, with normal vital signs. Mild left neck swelling and torticollis were noted, as was retrognatia, without facial dysmorphism. Auscultation revealed normal heart sounds with no cardiac murmurs. The breath sounds were clear, and the neurological examination was normal. The initial lab venous blood gas measurements were consistent with respiratory acidosis (pH 7.2, PCO2 67 mmHg, HCO3 - 24 mmHg), mild leukocytosis (15.9 103 /µL), and mild thrombocytosis (656 103 /µL). The glucose levels, electrolytes, and kidney function tests were normal, and the urine stick was negative for leukocytes. An electrocardiogram showed normal sinus rhythm.
The patient was admitted to the general pediatric department for further testing and evaluation of the neck mass and cyanotic episodes. A few transient episodes of cyanosis with desaturations of upto 75% in room air were documented upon arrival to the ward. A full neonatal sepsis evaluation, including blood, urine, and cerebrospinal fluid cultures, was performed in search for an infectious source, and empirical coverage with ampicillin and gentamycin was initiated. The working diagnosis included infectious conditions, congenital neck lesions (e.g., branchial cleft/thyroglossal duct cysts), neonatal seizures, and cardiovascular etiologies.
A cardiology consultation yielded no diagnostic evidence, and the infant underwent an echocardiogram for confirmation. A neurology consultation was also ordered with no clinical findings specific to neurological pathology, and the infant underwent an electroencephalogram and brain US. All of those studies were normal. A neck US, however, revealed a large cystic lesion whose dimensions on cross-section were 3.1 X 2.45 cm and about 4.3 cm in length. The lesion contained echogenic fluid extending from the region of the left thyroid lobe, posteriorly to the prevertebral aspect, and causing tracheal deviation to the opposite side. The thyroid isthmus and the right thyroid lobe were normal, and there was no cervical or mediastinal lymphadenopathy.
The patient was transferred to the pediatric intensive care unit due to impending airway obstruction. The initial endotracheal intubation attempt failed, and direct laryngoscopy revealed laryngeal deviation with a restricted laryngeal orifice. Successful endotracheal intubation was performed in the operating room by a pediatric anesthesiologist and a pediatric otolaryngologist. The patient needed minimal ventilatory support following intubation. After stabilization, a neck magnetic resonance imaging (MRI) study was performed for better identification of the US findings (shown in Figure 1A-C). A large cystic lesion was identified left to the midline of the neck, 4.2 cm in length and 2.73 cm width, extending from the upper cervical region, inferiorly along the cervical spine, and into the thoracic inlet, with an associated cervical kyphosis (shown in Figure 1B), together with a mass effect deviating the esophagus, trachea, and cervical blood vessels.
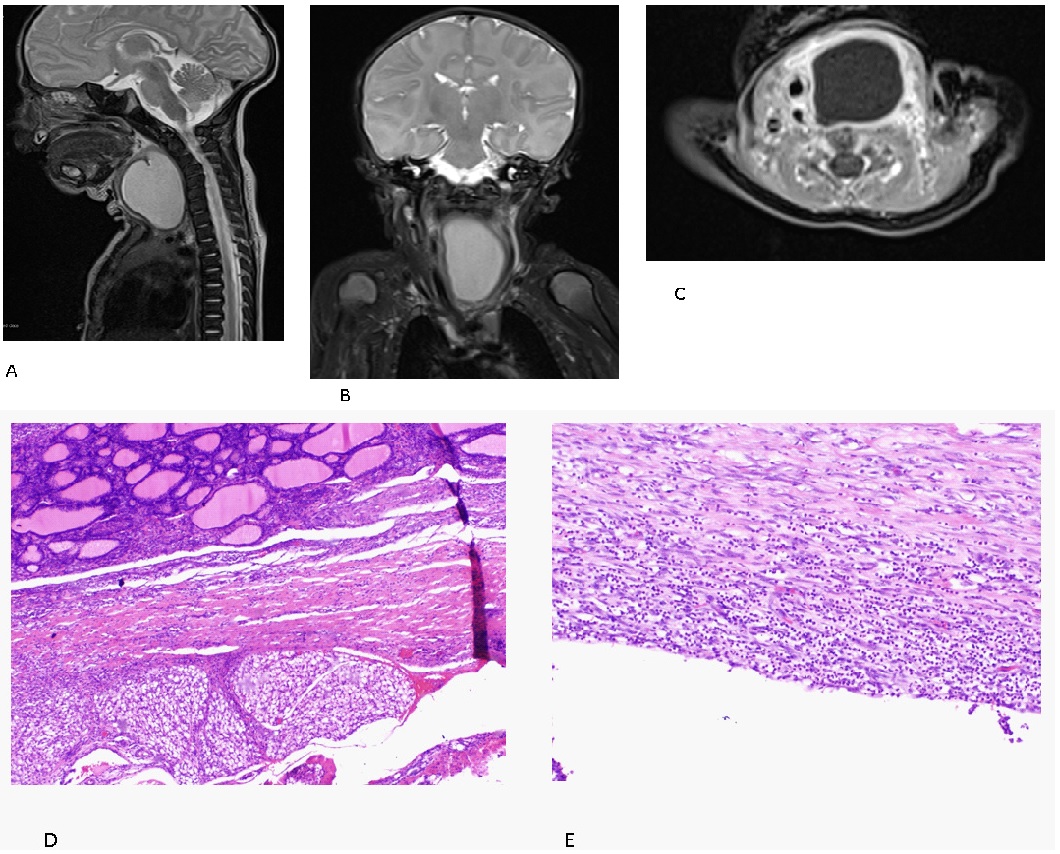
On the following day, the patient underwent total resection of the cyst by a pediatric otolaryngologist. The pathological report of the resected specimen confirmed the diagnosis of infected TGDC. A benign cystic lesion containing lymphoid and focal thyroid tissue together with heavy acute inflammation was observed (Figure 1D, 1E). The infant was successfully extubated on the second postoperative day, and he was transferred to the general pediatric department. He was discharged one week later free of respiratory symptoms, with a normal feeding pattern, and weight gain.
The postoperative follow-up in the pediatric otolaryngology outpatient clinic demonstrated reduced motility of the left vocal cord, both in endoscopy and in US. At 2 months of age, elevated Thyroid Stimulating Hormone (TSH) levels (TSH 13.2 mU/L) with normal free thyroxine (T4) levels (1.25 ng/dL [normal range 0.7- 1.80 ng/dL]) were detected. He underwent neck US at 3 months of age, and it demonstrated that the left thyroid lobe was smaller than the right one, with no evidence of cystic remnants. The patient was referred for endocrine consultation due to evidence of thyroid tissue in the excised cyst. Acquired hypothyroidism was diagnosed due to persistent elevated TSH levels with concomitant decrease in free T4 levels. Levothyroxine treatment at a dose of 25 mcg/d (3.8 mcg/kg/d) was initiated at 4 months of age with normalization of thyroid function under treatment. He is being regularly followed-up at the pediatric endocrine clinic. Now, at 2 years and 7 months of age, his thyroid function tests are within the normal range under treatment, linear growth is normal and similar to genetic height, and he has attained ageappropriate neurodevelopmental milestones.
Discussion
We report a newborn with an unusual presentation of TGDC. The clinical symptoms were subtle and unspecific, consisting of episodic cyanosis, eating difficulties, and mild neck swelling, thus yielding a wide range of options for differential diagnosis. The patient developed signs of upper airway obstruction and respiratory distress due to the rapidly enlarging neck mass, most probably due to superinfection that compressed the trachea and nearby blood vessels. This caused considerable difficulty in executing intubation due to the restricted laryngeal orifice, which is already narrow in a newborn. The advanced airway management was crucial in preventing life-threatening airway compromise in this child.
Cross-sectional imaging was performed in order to plan the appropriate surgical strategy. In our case, MRI was essential for the precise evaluation of the anatomical location and size of the lesion. Unexpectedly, the TGDC had an unusual location, extending to the thoracic inlet and positioned laterally to the midline. Most TGDCs are known to be situated in the midline, while 10% to 24% are located laterally, often to the left [4,5]. Surgical excision of the lesion was curative, and the histological examination of the excised specimen was consistent with infected TGDC. Hypothyroidism and reduced motility of the left vocal cord were detected postoperatively. In conclusion, TGDC is a rare etiology of airway compromise in the neonatal period. Whenever respiratory distress is accompanied by a neck mass, even when positioned laterally to the midline, a suspicion of TGDC should be raised and confirmation should be followed with the appropriate in-depth workup and intervention by a highly skilled team.
Acknowledgements: Our thanks to Esther Eshkol for editorial assistance.
Statement of ethics: The parents have given their written informed consent to publish their case.
Funding sources: No funding was secured for this study
Author contributions
Dr. Hejla and Dr. Elkon-Tamir collected data, carried out the initial analyses, drafted the initial manuscript, and reviewed and revised the manuscript.
Dr. Pratt, Dr. Wasserzug and Dr. Leider Trejo carried out the initial analyses, interpreted the data and critically reviewed and revised the manuscript for important intellectual content.
Dr. Brener and Prof. Lebenthal conceptualized and designed the study, and critically reviewed and revised the manuscript for important intellectual content.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
References
- Shah R, Gow K, Sobol SE. Outcome of thyroglossal duct cyst excision is independent of presenting age or symptomatology. Int J Pediatr Otorhinolaryngol. 2007; 71: 1731-1735.
- Chou J, Walters A, Hage R, et al. Thyroglossal duct cysts: anatomy, embryology and treatment. Surg Radiol Anat. 2013; 35: 875- 881.
- Foley DS, Fallat ME. Thyroglossal duct and other congenital midline cervical anomalies. Semin Pediatr Surg. 2006; 15: 70-75.
- Thompson LD, Herrera HB, Lau SK. A clinicopathologic series of 685 thyroglossal duct remnant cysts. Head Neck Pathol. 2016; 10: 465-474.
- de Tristan J, Zenk J, Künzel J, Psychogios G, Iro H. Thyroglossal duct cysts: 20 years’ experience (1992-2011). Eur Arch Otorhinolaryngol. 2015; 272: 2513-2519.