
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Laterally located mucocele in a hyperpneumatized frontal sinus causing exophthalmos: A total endoscopic approach
Charikleia Maiou*; Christos Korais; Eleni Gkrinia; Athanasios Saratziotis; Jiannis Hajiioannou; Charalampos Skoulakis
Department of Otorhinolaryngology, University Hospital of Larissa, Greece.
*Corresponding Author : Charikleia Maiou
ENT Surgeon, University Hospital of Larissa, Viopolis,
PC 41110, 1425, Larissa, Greece.
Email: hara_mai@hotmail.com
Received : Mar 02, 2021
Accepted : Apr 15, 2021
Published : Apr 17, 2021
Archived : www.jcimcr.org
Copyright : © Maiou C (2021).
Abstract
Frontal sinus mucoceles are mucous secretory lesions within the sinus, presenting a slow – growing pattern, mostly behaving like a space-occupying mass with subtle symptoms until a bone erosion of the surrounding structures takes place. Intracranial and intraorbital expansion are regarded as the most considerable complications, demanding adequate surgical management in order to avoid recurrence. Endoscopic drainage is thought to be the current treatment of choice, with external approaches or combined approaches being considered for more severe cases where anatomy and disease extension restricts adequate endoscopic visualization of the lesion.
We present a case of a 31-year-old female patient with a left frontal sinus mucocele, demonstrating with an unusual lateral frontal expansion and orbit invasion, causing exophthalmos and ophthalmoplegia. She was adequately managed by a Draf III endoscopic procedure achieving wide marsupialization and enough drainage of the mucocele. No sign of recurrence was noticed during the last 6-month follow-up.
Giant mucoceles of the frontal sinus are a rare pathology. To our knowledge, endoscopic endonasal approach is a treatment modality that can provide an adequate drainage pathway, thus resulting in optimal clinical outcomes, compared with external approaches.
Keywords: Frontal sinus; Mucocele; Exophalmos; Pneumosinus dilatans; Pneumocele.
Citation: Maiou C, Korais C, Gkrinia E, Saratziotis A, Hajiioannou J, et al. Laterally located mucocele in a hyperpneumatized frontal sinus causing exophthalmos. A total endoscopic approach. J Clin Images Med Case Rep. 2021; 2(2): 1052.
Introduction
Sinus mucoceles are benign pseudocystic lesions with mucous content that tend to expand slowly and often destructively to the adjacent structures [1]. The majority of mucoceles are located in the frontal sinus, followed by the ethmoids, whereas maxillary and sphenoid mucoceles are rare [2]. Imaging, including both CT and MRI, is essential for the diagnosis of mucoceles, and strictly necessary in case of possible complications [3] and, as in our case, anatomic variations or underlying pathology.
Surgical management is the treatment of choice, with the entirely endoscopic marsupializaton of the frontal sinus mucoceles representing the gold standard. The effectiveness of this technique is mainly based on the concept that there is no need to remove the mucocele lining. Prognosis is usually favorable, although a long follow up is recommended [4].
We report the case of a giant mucocele, presenting with exopthalmos and opthalmoplegia, located in an abnormally large and laterally expanded frontal sinus, that was adequately managed surgically by a total endoscopic approach.
Case presentation
A 31-year-old female was referred to our Department by the Ophthalmology Clinic, where she was hospitalized for unilateral left eye swelling along with proptosis and erythema (Figure 1,2). The patient had presented with a 2-day-onset of symptoms, progressing rapidly during the last 24 hours. She had no history of recent upper airway infection or trauma. Her medical history was pertinent for allergic rhinitis and she had no prior history of orbital, head or sinus surgery. The patient reported an incident of superficial head injury in the left supraorbital area 10 years ago, and recognized a mild unilateral left frontal bossing ever since.


Gross ophthalmologic examination revealed eyelid edema, non-action proptosis and hypotropia of the left eye. Best corrected visual acuities of 10/10 in both eyes were reported. Pupillary reflexes and color vision testing were normal. Ocular motility testing results were unremarkable concerning the right eye, whereas, in the left eye, ocular motility was restricted in abduction and in superior, superotemporal and superonasal fields of gaze. Diplopia was present in all the aforementioned positions, as well as in the primary gaze position of the involved eye.
The patient was in first place admitted in the ophthalmology clinic and, although laboratory blood testing revealed inflammation markers (CRP, ESR) within normal limits except for mild leukocytosis with neutrophilia, she was administered with broad spectrum intravenous antibiotics (ceftriaxone and clindamycin).
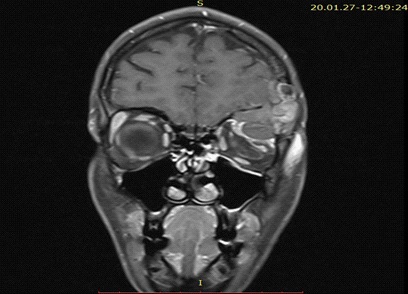
A Computed Tomography (CT) of the skull and the paranasal sinuses was performed demonstrating a markedly enlarged, laterally located and hyper –pneumatized left frontal sinus, occupied with an expansile hypodense lesion which partially eroded the floor of the frontal sinus (Figure 3). Invasion of the left orbit was depicted mainly in the superolateral aspect, with signs of compression of the superior rectus muscle. Noticeably, the superior and posterior wall of the left frontal sinus although relatively intact, they were markedly thinned. Subsequently, a Magnetic Resonance Imaging (MRI) was conducted, revealing the previously described mass, demonstrating no signs of intracranial extension and no dura enhancement (Figure 4,5).


Based on radiologic findings, the diagnosis of mucocele / mucopyocele was made and the patient was referred to the otolaryngology department for further management. Nasal endoscopy revealed a septum deviation and mild mucosa edema, with clear nasal discharge and no signs of acute sinusitis. A neurologic assessment was also performed presenting negative meningeal irritation signs.
Operative intervention was decided, including a navigationguided endoscopic sinusotomy, consisting of a Draf III procedure. A giant mucocele of the left frontal sinus was identified. The medial wall of its sac was incised and widely marsupialized with drainage of a large quantity of sero-purulent secretions. An artificial silicone frontal sinus stent was inserted to maintain adequate frontal sinus drainage patency. The histopathological examination confirmed the diagnosis of mucocele.
The patient underwent an uneventful postoperative course. Ocular motility and diplopia were remarkably improved the first postoperative day, returning to normal except for a slight restriction in the superior left eye movement (Figure 6). The patient was discharged on the third postoperative day. The ophthalmologic re-evaluation, 3 months postoperatively, revealed remaining minimal hypotropia. At 6 months postoperatively, however, this finding was absent, whereas the CT scan revealed a well aerated and free of lesions frontal sinus and a wide enough drainage pathway (Figure 7).


Discussion
Mucocele is a collection of mucoid secretions enclosed in a sac of lining sinus epithelium. It is a slow-growing condition; thus, it can take years to become symptomatic, mostly affecting the frontal sinus whereas the sphenoid, ethmoid and maxillary sinus involvement is quite rare [1]. According to Arrue P. et al, 60-89% occur in the frontal sinus, followed by 8-30% in the ethmoids and less than 5% in the maxillary sinus [2].
Mucoceles can be classified as primary, with no specific causal factor identified, or as secondary. Secondary mucoceles can be post-traumatic, iatrogenic or following radiotherapy. Nevertheless, the most acceptable pathogenetic mechanism of this entity is the nasal ostium obstruction, causing subsequent impairment of the sinus drainage, establishing a chronic inflammatory status [6]. Recent data from the literature support the theory that mucoceles are able to expand themselves and can be locally destructive due to a bone-remodeling process of reabsorption and neogenesis between the mucocele and the surrounding bone which is exacerbated by the pressure applied by the mucocele itself on the bony tissue [7]. Previous research has demonstrated that high levels of prostaglandin E2 plays a major role in this osteolytic process and explains the locally aggressive behavior of mucoceles [8].
The frontal sinus, unlike other sinuses, is absent at birth and it begins forming after the second year of life. A variety of pathological entities may influence the development of the frontal sinus, leading to an abnormally expanded and aerated sinus which has been addressed in the literature as hypersinus, pneumosinus dilatans or pneumocele [9]. These anatomical variants refer to enlarged and aerated sinuses which is either limited in the normal bony walls of the frontal bone, in case of hyper-(pneumatized)-sinus, or abnormally expanded beyond the normal boundaries of the frontal bone, in case of pneumosinus dilatans and pneumocele. Although these last two unusual processes in the frontal bone present with similar clinical symptomatology like frontal bossing, local pressure symptoms and most of the times orbital encroachment, there is a unique feature that differentiates them. Pneumosinus dilatans presents with expanded but intact sinus bony walls whereas pneumocele has lost its normal bony thickness leading to bony erosion [10]. Both the CT findings and clinical examination are mandatory in order to classify an aerated sinus into one of the aforementioned categories. In our case, although the patient had been asymptomatic, she reported a recognizable mild frontal bossing at the left side, possibly associated with the enlarged left frontal sinus, supporting the diagnosis of pneumosinus dilatans or pneumocele.
The relationship between a hyperpneumatized frontal sinus and the development of a mucocele remains currently unknown, but possibly share common pathophysiology. The dominant theory is the mechanism of increased intra-sinus pressure in both conditions, as well as the secondary development of a pneumocele due to spontaneous drainage of a pre-existing mucocele [11].
Because of the close anatomic relation of the frontal sinus with the orbit and brain, intraorbital and intracranial spread are thought to be the most considerable complications. Proptosis (83%) and diplopia (45%) are the most common symptoms when the bony floor of the frontal sinus is eroded, and the orbit is affected. Decreased visual acuity and restriction of extraocular movements can be also detected [3]. Severe headaches, fever, meningitis and CSF fistula can be developed once the posterior wall of the frontal sinus is involved, and intracranial extension is present [4].
Except history and physical examination, radiological assessment is essential for the diagnosis. A CT scan, in most of the cases, demonstrates a homogenous mass, with clearly defined margins causing expansion of the sinus and thinning or erosion of the bony sinus walls. However, this space-occupying lesion may sometimes imitate other sinonasal neoplasms, thus making MRI helpful in establishing a definite diagnosis [5]. Typically, mucoceles tend to appear bright on T1W images and iso-hyperintense on T2W images [6]. However, differentiating secretions from other proteinaceous content of a lesion is not always possible using a gadolinium-enhanced MRI. In such complicated cases, CT and MRI are usually complementary [12].
Surgical intervention is the treatment of choice for mucoceles. Because many of the mucoceles have an intracranial or intraorbital extension, it is preferable to operate on a non-infected sinonasal status, unless the procedure is performed for acute symptomatic mucopyocele [13].
According to literature, external approaches, such as cranialization or osteoplastic flaps with sinus cavity obliteration, were the generally preferred treatment modalities the previous years [14]. With the introduction of endoscopic sinus surgical paradigm, there has been a recent trend towards transnasal endoscopic management of frontal mucoceles. Instead of radical procedures, endoscopic drainage of the mucocele along with maintenance of an open frontal recess with sufficient sinus ventilation is the preferred treatment modality. A total endoscopic intervention provides reduced overall mortality rates, leaves no scars and preserves sinus architecture. In our case a total endoscopic approach was decided, considering the young age of the patient, in order to avoid facial scarring, despite potential difficulties because of the underlying anatomic frontal sinus variation.
Conclusion
Mucoceles are pseudocystic lesions with mucous content causing gradual expansion and erosion of the surrounding bony walls, often manifestating with orbital complications. The association between the hyperpneumatization of the frontal sinus and the development of mucocele still remains ambiguous, according to existing literature. Transnasal endoscopic marsupialization seems to be the current surgical method of choice for the management of frontal sinus mucoceles, whereas transcranial or transfacial approaches represent treatment modalities for more extended and complexed lesions where endoscopic techniques cannot be applied.
References
- Devars du Mayne M, Moya-Plana A, Malinvaud D, O Laccourreye, P Bonfils. Sinus mucocele: natural history and long-term recurrence rate. Eur Ann Otorhinolaryngol Head Neck Dis 2012; 129: 125-130.
- Arrue P, Kany MT, Serrano E, Lacroix F, Percodani J, et al. Mucoceles of the paranasal sinuses: Uncommon location. J LaryngolOtol. 1998; 112: 840-844.
- Tan CS, Yong VK, Yip LW, Amritj S. An unusual presentation of a giant frontal sinus mucocele manifesting with a subcutaneous forehead mass. Ann Acad Med Singapore 2005; 34: 397-398.
- Voegels RL, Balbani AP, Santos Junior RC, Butugan O. Frontoethmoidal mucocele with intracranial extension: A case report. Ear Nose Throat J. 1998; 77: 117-20.
- Galiè M, Mandrioli S, Tieghi R, Clauser L. Giant mucocele of the frontal sinus. J Craniofac Surg 2005; 16: 933-935
- Edelman RR, Hesselink JR, Zlatkin MB, Crues JV. Clinical Magnetic Resonance Imaging. 3rd ed. Philadelphia: Elsevier. 2006. p. 2035-7
- Terranova et al. Bone Regeneration After Sinonasal Mucocele Marsupialization: What Really Happens Over Time? The Laryngoscope 2015; 125: 1568-1572
- Lund VJ, Harvey W, Meghji S, Harris M. Prostaglandin synthesis in the pathogenesis of fronto-ethmoidal muco-coeles. Acta Otolaryngologica, 1988; 106: 145-151.
- Uddstromer L. The osteogenic capacity of tubular and membranous bone periosteum. A qualitative and quantitative experimental study in growing rabbits. Scand J Plast Reconstruct Surg 1978; 12: 195–205.
- Urken ML et al. Abnormally large frontal sinus. II. Nomenclature, pathology, and symptoms. Laryngoscope, 1987; 97: 606-611.
- Lund VJ. Fronto-ethmoidal mucoceles: A histopathological analysis. J LaryngolOtol 1991; 105: 921-923.
- Lanzieri CF, Shah M, Krauss D, Lavertu P. Use of gadoliniumenhanced MR imaging for differentiating mucoceles from neoplasms in the paranasal sinuses. Radiology. 1991; 178: 425.
- Sushil Kumar Aggarwal, Kranti Bhavana, Amit Keshri, Raj Kumar, Arun Srivastava. Frontal sinus mucocele with orbital complications: Management by varied surgical approaches. Asian J Neurosurg. 2012; 7: 135-140.
- Rubin JS, Lund VJ, Salmon B. Frontoethmoidectomy in the treatment of mucoceles: A neglected operation. Arch Otolaryngol Head Neck Surg. 1986; 112: 434-436