
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Ultrasound guided femoral artery cannulation: A key point for security
Niño Claudia1*; Useche Nicolas2; Amaya-Zuñiga William1
1 University Hospital of the Santa Fe de Bogotá Foundation, Anesthesia, Colombia
2 University Hospital of the Santa Fe de Bogota Foundation, Radiology, Colombia.
*Corresponding Author : Niño Claudia
University Hospital of the Santa Fe de Bogotá
Foundation, Anesthesia, Colombia.
Email: gigi87@yahoo.com
Received : Mar 05, 2021
Accepted : Apr 16, 2021
Published : Apr 21, 2021
Archived : www.jcimcr.org
Copyright : © Claudia N (2021).
Citation: Claudia N, Nicolas U, William AZ. Ultrasound guided femoral artery cannulation: A key point for security. J Clin Images Med Case Rep. 2021; 2(2): 1055.
Case report
Some meta-analyses have shown the broad benefits of the ultrasound visualization for arterial cannulation, such as the increases of the first-attempt success rate, mean attempts, meantime, and reduction of hematoma incidence. The advantages over the palpation technique, promote the inclusion of ultrasound guide as part of the recommendation for arterial cannulation [1].
The arterial access in the pediatric and neonatal population represents a challenge in the anesthesia and critical care scenarios. The small diameter of the vessels and some pathological disorders require new strategies for successful process improvement [2].
Invasive monitoring, blood samples collection in multiple scenarios as the emergency department, operation room, critical care, and hemodynamic laboratory necessitate the use of femoral artery lines. Even though complications remain infrequent (3.5%), these can be severe (10.5%), sometimes require surgical intervention and blood transfusion (6.4%), as well as increase the mortality (4.7%) [3].
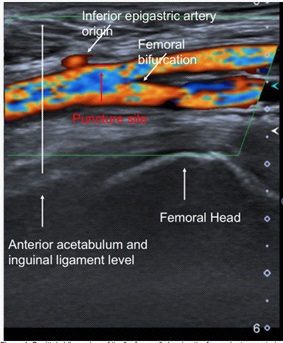
We recommend ultrasound-guided cannulation of the femoral artery always to reduce the risk of complications. A too distal puncture of the femoral artery, at the femoral bifurcation, could cause an anterior wall lesion and predisposes to the formation of pseudoaneurysms. This consideration is particularly critical in obese and edematous patients in which the inguinal crease is caudally displaced. On the other hand, a very high puncture of the femoral artery, above the inguinal ligament, predisposes the risk of retroperitoneal hematoma and hidden hemorrhage in a noncompressible zone, a rare but life-threatening complication. This circumstance is more frequent when the artery’s posterior wall has inadvertently trespassed in an anticoagulated patient. This situation can be avoided using ultrasound that allows the permanent visualization of the needle and the puncture of only the anterior wall. We recommend using the femoral head as a landmark of the safe zone for ultrasound-guided puncture. In a sagittal oblique view, the femoral artery is anterior to the femoral head’s superomedial edge. In this position, the bifurcation is seen as inferior, preventing a too distal puncture [4,5]. The anterior border of the acetabulum and pelvic ring superior and are the landmarks for the inguinal ligament, avoiding very proximal access. Identifying the origin of the inferior epigastric artery is critical to prevent its injury with the risk of a pseudoaneurysm. Sometimes the space for puncture is limited, as is shown in the image (Figure 1).
This safe zone has another advantage, when the vascular sheath or catheter is removed, the artery is compressed efficiently over a posterior hard and bony surface. All these advantages also apply to infants and children. Interventional radiologists described this concept for fluoroscopic guidance, but it can be extrapolated to the ultrasound guidance. Therefore, we propose using the femoral head as an ultrasound reference to be used in adult and pediatric patients to reduce complications and improve patient safety.
References
- Jang YE, Ji SH, Kim EH, Lee JH, Kim HS, et al. Subcutaneous Nitroglycerin for Radial Arterial Catheterization in Pediatric Patients: A Randomized Controlled Trial. Anesthesiology. 2020; 133: 53- 63.
- Cuper NJ, de Graa JC, Hartman BJ, Verdaasdonk RM, Kalkman CJ. Difficult arterial cannulation in children: Is a near-infrared vascular imaging system the answer? Br J Anaesth. 2012; 109: 420-426.
- Troianos CA, Hartman GS, Glas KE, et al. Special articles: Guidelines for performing ultrasound guided vascular cannulation: Recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. Anesth Analg. 2012; 114: 46-72.
- Sobolev M, Slovut DP, Lee Chang A, Shiloh AL, Eisen LA. Ultrasound guided catheterization of the femoral artery: A systematic review and metaanalysis of randomized controlled trials. J Invasive Cardiol. 2015; 27: 318- 323.
- Pitta SR, Prasad A, Kumar G, Lennon R, Rihal CS, et al. Location of femoral artery access and correlation with vascular complications. Catheter Cardiovasc Interv. 2011.