
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A case of syphilis with an extremely high RPR titer
Luqman Dabiri
Port Orange Internists, Port Orange, FL 32217, USA.
*Corresponding Author : Luqman Dabiri
Port Orange Internists, Port Orange, FL 32217,
USA.
Email: lkdabiri@yahoo.com
Received : Mar 10, 2021
Accepted : Apr 19, 2021
Published : Apr 22, 2021
Archived : www.jcimcr.org
Copyright : © Dabiri L (2021).
Abstract
It remains unidentified why this patient has an extremely high Rapid Plasma Reagin Titer (RPR) 1: 2048. A false positive result was ruled out by a Treponemal test. To ensure accuracy, repeat tests were requested for both the Non-Treponemal and Treponemal Tests in the same laboratory, and the results came back the same. In the Traditional Algorithm, Positive Nontreponemal Syphilis screening tests are confirmed by Treponemal tests, although the latter is not quantitative. The lack of full sensitivity in the Traditional Algorithm Testing has led the CDC and some other centers to adopt Reverse Sequence Testing.
The resurgence of syphilis after 20 years could lead to mutagenic strain thus making it relevant for a need for heightened awareness.
Keywords: Syphilis; Extremely high RPR titer; Treponema pallidum; Resurgence; Mutagenic strain; Syphilitic cervicitis.
Citation: Dabiri L. A case of syphilis with an extremely high RPR titer. J Clin Images Med Case Rep. 2021; 2(2): 1058.
Introduction
The Center for Disease Control and Prevention [1] reports a resurgence of Syphilis, with the highest rate within the last 20 years. The CDC also reported outbreaks of Syphilis in many cities in the US.
Syphilis can affect multiple organ systems, cause numerous complications and could be fatal if untreated. It can be vertically transmitted to the fetus causing congenital anomalies and even stillbirths. Syphilis can lead to facilitation and transmission of Human Immunodeficiency Virus.
An incidental finding of extremely high RPR (Rapid Plasma Reagin) titer of 1: 2048 was found in a woman with Latent Syphilis. The patient was also positive for Hepatitis A Virus (HAV), Hepatitis B Virus (HBV) Core Antibody, Hepatitis B Surface Antibody and Hepatitis C Virus (HCV). There was a history of Latent Tuberculous Infection (LTBI) in 2003, treated with Isoniazid. The patient has a high-risk behavior for prostitution, and intravenous drugs abuse, and this is her sixth episode of incarceration. While the cause of this atypical and highly elevated RPR might be unknown, an attempt is made to review the anomalous immunological behavior of Syphilis (duality of immune evasion and immune recognition) and HCV (hepatocellular injury rather than cell death, which promotes chronicity and prolonged immune response), and the fact that environmental and climatic stresses are known causes of mutation. Mathematical Biosciences postulates that the ‘combined host–parasite dynamics is a multifaceted system that involves numerous scales of time, space, and biological components and processes’ [2].
This paper acts as an eye-opener for physicians, and to encourage further research and awareness for possible disease reactivation or mutation/immune modulation.
Case report
55yo W/F G3P3, motel housekeeper, on her sixth episode of incarceration. An extremely high RPR 1: 2048 was noted on the initial lab intake. Because this was extremely high, another specimen was sent to the same lab (Bioreference Laboratory Inc, Genpath Diagnostics) for repeat RPR test one week after, and found to be the same value. Reflex Treponema pallidum test was positive in both instances - Bioreference; Chemiluminescence immunoassays (CIAs).
Review of records all the five previous incarcerations revealed negative RPR test results. The patient denied any history suggestive of any sore or chancre (suggestive of Primary Syphilis) but confirmed that she observed a firm, painless sore on the penis of the partner. The patient is aware that partner has at least six other sexual partners). The patient denied a history of diffuse rash on the body, mouth or vagina or any such ailment in the palm and soles that might be typical of Secondary Syphilis. The patient did not describe any neurological or cardiac clinical features to suggest Tertiary Syphilis.
During the previous incarceration in 2003, she received Isoniazid treatment for Latent Tuberculous Bacilli Infection.
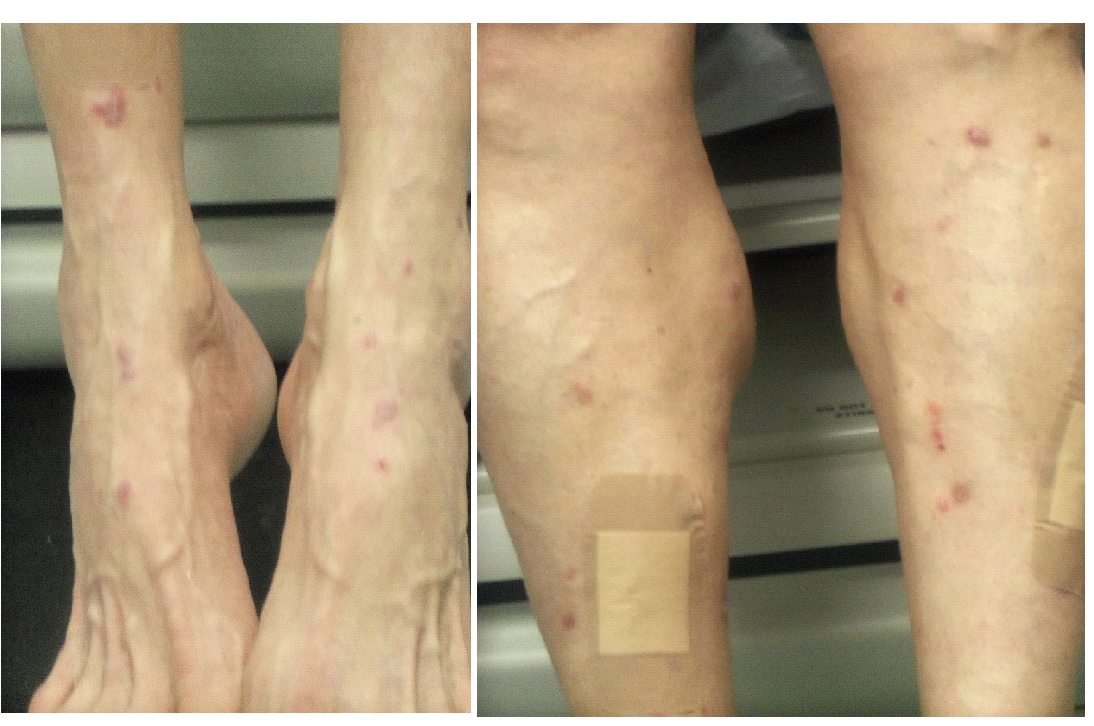
The patients Physical Examination exam was unremarkable, except for multiple rashes noted on both legs, mainly on the anterior and lateral aspect of the legs and the dorsum of the feet but sparing the posterior legs and plantar of the feet (Figure 1). There were no similar rashes in the palm, upper limb, trunk, head or neck.
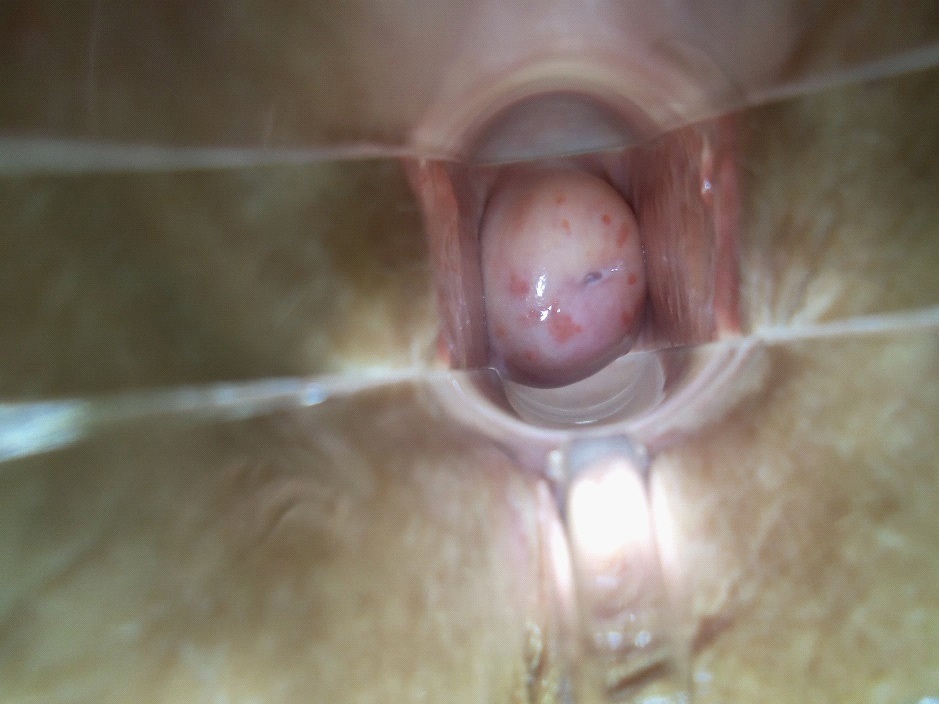
Examination of the pelvis and perineum and vulva did not reveal any rash, chancre, typical syphilitic sore or gumma. There was no lesion in the anus. Speculum examination and colposcopy of the vagina and cervix showed 15-20 scattered, slightly raised flat-topped, erythematous lesions of varying size on the cervix (see Figure 3). Digital pelvic and rectal exams were negative.
This patient was treated as a case of Latent Syphilis (serological evidence of syphilis without clinical manifestations) and had 2.4 mU of intramuscular Bicillin weekly for three weeks. The lesions on the leg and cervix were biopsied to confirm syphilis.
The Dermatologist could not assign the skin rashes on the legs to syphilis but a differential diagnosis of Lichen Simplex Chronicus, Prurigo was entertained. Optometry evaluation ruled out uveitis, iritis or other features that might be suggestive of Tertiary Syphilis.
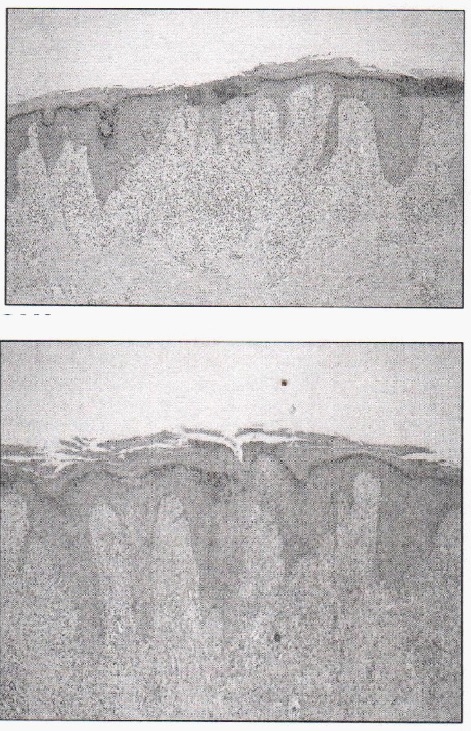
The lesions on the cervix and the legs were respectively biopsied to rule out secondary syphilis or other differentials. The biopsies were done to include a rim of healthy tissue to ensure proper comparison of normal to abnormal tissue. The skin histopathology revealed Lichenoid dermatitis. Though immunostaining was Acid Fast Bacilli (AFB) negative and spirochete negative, an infectious process such as treated syphilis could not be ruled out (the patient was treated promptly before the biopsy was done). The histopathology of cervical lesions showed: focal acute and chronic inflammation, negative for dysplasia; no spirochetes were seen on immunostaining.
Other relevant lab results include: PAP smear was Negative for Intraepithelial Lesion or Malignancy (NILM), with no Human Papilloma Virus (HPV) detected. Urine by Genotype Aptima test for N. Gonorrhea and C. Trachomatis were negative. Human Immunodeficiency Virus (HIV) test was negative. HbA1c was 5.1 %. The patient was positive for Hepatitis A virus (HAV), Hepatitis B virus (HBV), Hepatitis C virus (HCV). The Hep C RNA viral load count was 3,073 IU/mL, genotype 1a, and Fibrotest score was F4 (severe fibrosis). Due to the history of LTBI, a chest X-ray was repeated but did not reveal active TB.
Discussion
This extremely high titer exhibited by this patient is hard to explain and might be due to yet unknown phenomena. False positive Non-Treponemal Tests can occur in auto-immune and chronic inflammatory conditions, are usually with a titer of less than 1:8; however, the Treponemal Test result will be negative. Both Non-Treponemal and Treponemal tests can yield falsenegative results due to the prozone phenomenon. While not discountenancing HAV, HBV and LTBI, an attempt is being made to review the unique immunobiology Syphilis and HCV, as correlated to possible immune modulation [3,4].
The lack of a vaccine for Syphilis underscores our poor understanding of T. pallidum immunobiology. Syphilis continues to confound despite being discovered in 1905 by Schaudinn and Hoffman [5]. Its protean presentation led to titles like ‘the Great Mimicker,' ‘the Stealth Pathogen' [6,7]. Syphilis has been increasing dramatically worldwide since 2000 [1]. Bloodborne STD’s – Syphilis, Hepatitis B virus (HBV), hepatitis C virus (HCV) and Human Immunodeficiency Virus (HIV) have a prevalence of about 2-10 times higher in the prisons and the jails than the general population. This might possibly be due to drugs and high-risk sex-related behaviors practiced outside Correctional settings; however, the transmission has been documented inside jails and prisons also [8-10].
Treponema pallidum subspecies pallidum is an exclusively a human pathogen, with a small genome and possibly utilizes host biosynthesis for its metabolic needs [6]. The host-parasite interaction in syphilis infection evokes a complex immune reaction, in which the humoral immunity plays a minor role as compared to cellular. It has been shown that some form of anergy exists in the initial stages permitting early dissemination and immune evasion [7,11]. Cruz and others [12], was able to demonstrate the paradox of immune evasion and simultaneous immune recognition with an ability to induce inflammation. It is also known that autoimmune response has been triggered due to a secondary reaction to T. pallidum, with the production of various antibodies to self-antigens [13].
Immunobiology of HCV with research assays capable of detecting HCV RNA at sensitivities superior to those offered by clinical assays has significantly contributed knowledge of HCV reactivity in the hepatocyte, plasma/serum, and peripheral lymphomononuclear cells. It shows that HCV mainly causes injury to the infected hepatocytes, rather than cell death, and thereby promoting lymphotropism, occult persistence, and chronicity. The consequent prolonged and profound immune response is associated with the breaching of immune tolerance which may lead to a higher prevalence of immunological processes [14]. While some of these immune responses are well documented [15], a lot may still be unknown.
Environmental and climatic stresses are known mutagens. It has been implicated in the mutagenesis of bacteria [16,17] and influenza virus and its outbreaks [18]. It was environmental stress factors that led to mutations that earned the Zika Virus a terrible reputation. It was previously a tepid virus before becoming toxic, due to clinically significant mutation [19]. Recent case reports of by Divyani and others [19] and Liu and others [20] indicates atypical presentations of Syphilis might not be as rare as we thought. The presentation of Syphilis as a case of pure cerebellar ataxia indicates that mutagenic presentations go undetected for a long time and that we should continue to be vigilant in detecting unusual association of diseases and symptoms [20]. Liu reported unusual constellation of symptoms and outpatient diagnosis of syphilis [21], in 2015,
Zhu and others reported a rare case of syphilis presenting as syphilitic cervicitis, RPR of 256. The spirochetes were not able to be identified in the lesion, at the time of presentations., similar to this reported case (though we started treatment promptly before the biopsy was done). Neither did not have external genitalia lesions but both cervical lesions that shows chronic inflammatory cells on histopathology.
This paper highlights a case of an extremely high titer confirmed by non-treponemal tests, rashes mainly in the anterior leg and dorsum of the feet (noted on histopathology that chronic infection like syphilis cannot be ruled out), multiple elevated rashes in the cervix may well be an atypical presentation of syphilis or perhaps an insignificant or yet unknown mutation of a re-emerging and resurging spirochete- an old foe that was 4th most significant cause of death before WWII .
The CDC has confirmed resurgence of syphilis after a long quiescence, recent reports of atypical presentation suggest mutagenesis.
References
- Division of STD Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention. Sexually Transmitted Diseases Surveillance Report-CDC. 2016; 2017. https://www.cdc.gov/std/stats16/Syphilis.htm
- Editorial, Mathematical Biosciences. Part B. 2015; 270: 143-155.
- Ratnam S. The laboratory diagnosis of syphilis. Can J Infect Dis Med Microbiol. 2005; 16.
- Surajit Nayak and Basanti Acharjya. VDRL Test and its Interpretation. Indian J Dermatol. 2012; 57: 3-8.
- Morshed MG. Current trend on syphilis diagnosis: issues and challenges. Adv Exp Med Biol. 2014; 808: 51-64.
- Peeling RW, Hook EW 3rd. The pathogenesis of syphilis: The Great Mimicker, revisited. J Pathol. 2006; 208: 224-232.
- Radolf JD, Deka RK, Anand A, Šmajs D, Norgard MV, Yang XF. [[6]]. Treponema pallidum, the syphilis spirochete: making a living as a stealth pathogen. Nat Rev Microbiol. 2016; 14: 744-759.
- Kahn RH, Scholl DT, Shane SM, Lemoine AL, Farley TA. Screening for syphilis in arrestees: usefulness for community-wide syphilis surveillance and control. Sex Transm Dis. 2002; 29: 150-156.
- Weinbaum CM, Sabin KM, Santibanez SS. Hepatitis B, hepatitis C, and HIV in correctional populations: a rev iew of epidemiology and prevention. AIDS. 2005; 19: S41-S46.
- Adjei AA, Armah HB, Gbagbo F, Ampofo WK, Quaye IK, Hesse IF, et al. Prevalence of human immunodeficiency virus, hepatitis B virus, hepatitis C virus and syphilis among prison inmates and officers at Nsawam and Accra, Ghana. J Med Microbiol. 2006; 55: 593-597.
- Pavia CS, Folds JD, Baseman JB. Cell-mediated immunity during syphilis. A review Br J Vener Dis. 1978; 54: 144-150.
- Cruz AR, Ramirez LG, Zuluaga AV, Pillay A, Abreu C, Valencia CA, et al. Immune Evasion and Recognition of the Syphilis Spirochete in Blood and Skin of Secondary Syphilis Patients: Two Immunologically Distinct Compartments. PLoS Negl Trop Dis. 2012; 6: e1717.
- Wicher K, Wicher V. Autoimmunity in syphilis. Immunol Ser. 1990; 52: 101-124.
- Huang L, Koziel MJ. Immunology of hepatitis C virus infection. Curr Opin Gastroenterol. 2000; 16: 558-564.
- Calvaruso V, Craxì A. Immunological alterations in hepatitis C virus infection. Br J Vener Dis. 1978; 54: 144-150.
- Bjedov I, Tenaillon O, Gérard B, Souza V, Denamur E, Radman M, et al. Stress-induced mutagenesis in bacteria. Science. 2003; 300:1404-1409
- Wolf DM, Vazirani VV, Arkin AP. Diversity in times of adversity: probabilistic strategies in microbial survival games. J Theor Biol. 2005; 234: 227-253.
- Sooryanarain H, Elankumaran S. Environmental role in influenza virus outbreaks. Annu Rev Anim Biosci. 2015; 3: 347-373.
- Garg D, Vibha D, Pandit AK, Srivastava AK. Neurosyphilis presenting as pure cerebellar ataxia: an atypical manifestation. CASE REPORT: Unusual association of diseases/symptoms. BMJ Case Reports. BMJ Journals. 2019; 12.
- Zhu X, Zhang W, Fei J, Zhou J. Cervical syphilitic lesions mimicking cervical cancer: a rare case report. International Journal of Infectious Diseases. 2015; 31: 1-3.
- Liu E, Newbury-Palma E, Taylor J, Izokaitis A. P722 An unusual constellation of symptoms: outpatient diagnosis of neurosyphilis with no history of prior syphilis symptoms. Sexually Transmitted Infections. 2019; 95: A313.