
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Atlas of 99mTc-HMPAO SPECT brain perfusion in pediatric brain disorders
Saleh A Othman
Department of Radiology and Medical Imaging, King Khalid University Hospital and College of Medicine, King Saud University, 7805(46), Riyadh 11472, Saudi Arabia.
*Corresponding Author : Saleh A Othman
Department of Radiology and Medical Imaging,
King Khalid University Hospital and College of
Medicine, King Saud University, 7805(46), Riyadh
11472, Saudi Arabia.
Email: sothman@ksu.edu.sa
Received : Mar 11, 2021
Accepted : Apr 19, 2021
Published : Apr 22, 2021
Archived : www.jcimcr.org
Copyright : © Othman SA (2021).
Abstract
Background: Blood flow to the brain is in parallel with brain metabolism in almost all brain disorders except in brain tumors and therefore regional cerebral blood flow can be used as a marker of metabolic brain activity and hence it is closely linked to neuronal activity, the activity distribution is presumed to reflect neuronal activity levels in different areas of the brain.
Purpose: The aim of this work is to demonstrate to pediatrician in general and pediatric neurologist in particular the variations in cerebral perfusion during normal development which should be taken into consideration at the time of interpreting SPECT brain perfusion scan in different pediatric brain disorders.
Method: Brain SPECT was performed 10 minutes after an intravenous injection of 11.1 MBq/kg (0.3 mCi/kg), and the minimum dose is 185 MBq (5 mCi) of 99mTc-HMPAO (4).
Results: This was a retrospective analysis of SPECT brain perfusion scan of pediatric patients performed between October 2015 and December 2019 at our institution. We selected normal and abnormal studies in pediatric population with age range (5 months - 14 years).
Conclusion: Although anatomic cross sectional imaging give details of neurological structural changes, SPECT perfusion mirrors indirectly both metabolic and neuronal activity changes. Therefore, accurate interpretation of SPECT perfusion will consolidate its role as part of the diagnostic protocol and used when the findings of other imaging modalities do not explain the symptoms or fail partially or completely in determining the etiology of brain disorders in pediatric patients.
Keywords: Blood; Brain disorders; Tumors; Cerebral blood flow; Injection.
Abbreviations: ADHD: Attention Deficit Hyperactivity Disorder; MMD: Moyamoya Disease; RCBF: Regional Cerebral Blood Flow; SPECT: Single-Photon Emission Computed Tomography; 99mtc-HMPAO: Technetium-99m-Hexamethylpropyleneamine Oxime; 99mtc-ECD: 99mtc-Ethylene Cysteine Diethylester.
Citation: Othman SA. Atlas of 99mTc-HMPAO SPECT brain perfusion in pediatric brain disorders. J Clin Images Med Case Rep. 2021; 2(2): 1061.
Background
Blood flow to the brain is in parallel with brain metabolism in almost all brain disorders except in brain tumors and therefore regional Cerebral Blood Flow (rCBF) can be used as a marker of metabolic brain activity [1] and hence it is closely linked to neuronal activity, the activity distribution is presumed to reflect neuronal activity levels in different areas of the brain. Furthermore, (rCBF) has been described to reflect brain development and can be used to assess behavior changes in early childhood [2].
Brain perfusion can be assessed with different techniques including Nuclear Medicine (NM) Imaging and MRI studies. Single-Photon Emission Computed Tomography (SPECT) Imaging is a functional nuclear imaging technique performed to evaluate (rCBF). The most commonly used brain perfusion imaging agents are technetium-99m-hexamethylpropyleneamine oxime (99mTc-HMPAO) and 99mTc-ethylene cysteine diethylester (99mTc-ECD) with a half-life of 6.02 hours. Both are sensitive indicators of (rCBF) changes and can detect changes in blood flow overtime or immediately after an acute event [3].
The aim of this work is to demonstrate the variations in cerebral circulation and metabolism during normal development which should be taken into consideration at the time of interpreting SPECT brain perfusion scan performed to evaluate brain disorders in children and infants.
Materials and methods
Brain SPECT scanning to evaluate regional cerebral blood flow was performed 10 minutes after an intravenous injection of 11.1 MBq/kg (0.3 mCi/kg), and the minimum dose is 185 MBq (5 mCi) for both brain-specific agents [4]. The injection was made within 30 minutes after kit preparation.
Patients were positioned supine in supine with the head in a head holder and/or secured with a velcro strap to prevent motion. The head is flexed so that the cerebellum is included in the field of view. Imaging room should be quiet and dimly lit.
Imaging was performed using a dual head gamma rotating, large field-of view
(Philips’ BrightView XCT) fitted with a low-energy and high resolution collimator. Sixty four images were acquired for 20 seconds each, during a 360° camera rotation. Each image was stored in a 64 X 64-pixel matrix. Reconstruction of the image was performed with attenuation correction, using Hanning filters to produce transverse, sagittal, and coronal images [5,6].
Results
This was a retrospective analysis of SPECT brain perfusion scan performed at our institution for pediatric patients between Oct. 2015 and December 2019.
We selected normal and abnormal SPECT perfusion studies in pediatric and children population with age range (5 months - 14 years).
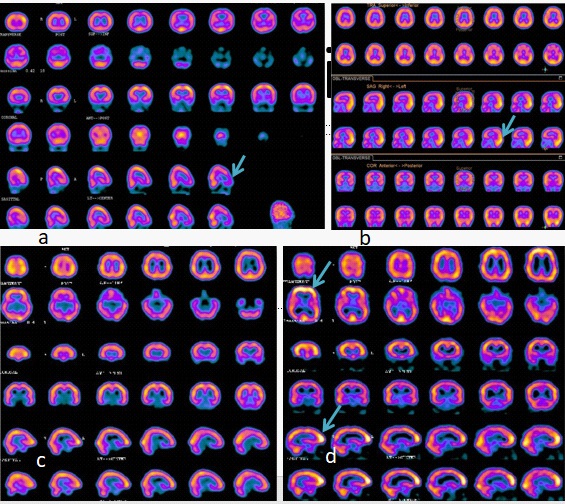
Variations in cerebral circulation (Figure 1a-d) and metabolism during normal development must be taken into consideration at the time of interpreting SPECT brain perfusion scan performed to evaluate any brain disorders in children and infants [4].
In this work we will illustrate the different patterns of (rCBF) in common and rare neurological pediatric disorders.
Epilepsy
SPECT brain scan in epilepsy is the most commonly NM procedure performed in neurological disorders in children. Patients with intractable and refractory disease are amenable to surgical treatment. Those selected for surgery should have in addition to clinical examination different investigations including Electroencephalogram (EEG), Magnetic Resonance Imaging (MRI), Positron Emission Tomography (PET) and brain SPECT to localize the epileptic focus [5,6].
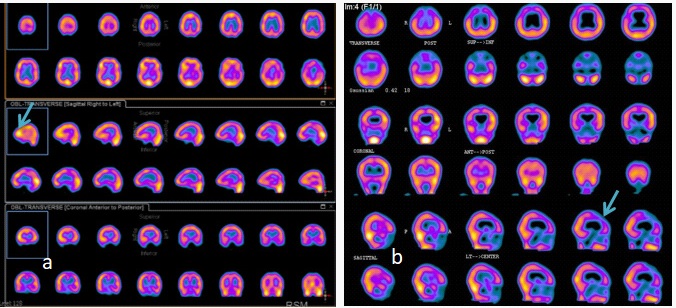
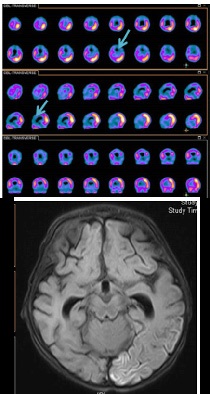
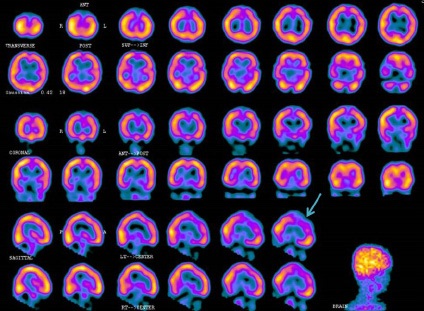
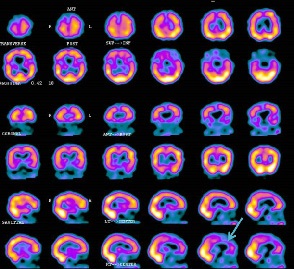
The scintigraphic patterns of brain SPECT in epilepsy differ whether performed during ictal or interictal phase showing increased uptake in the former (Figure 2a) and decreased uptake in the latter (Figure 2b).
Non-epileptic causes of seizure
A non-epileptic seizure is defined as a transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain due to previous brain insult [7].
Certain types of seizure disorders are likely to be associated with structural brain lesions, including tumors, infection, infarction, traumatic brain injury, vascular malformations, developmental abnormalities, and other brain pathology [8]. A cause is identifiable in less than 20% of children with seizures [9].
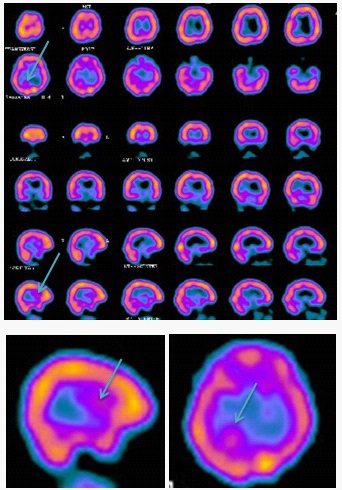
Patients without a provoked cause of first seizure require further evaluation. Contrast enhanced CT of the brain is useful as initial investigation. MRI can depict subtle abnormalities that may go unrecognized on CT. Refractory epilepsy requires special tests such as EEG, SPECT and PET studies. Herein we will review the different scan patterns of SPECT scan in non-epileptic secondary seizures (Figure 3a-e).
Developmental disorders
Advanced imaging techniques have provided a new horizon into a relationship between the neuronal activity and brain development disorders. SPECT brain scan was one of these promissing techniques. In this review we will show the expected patterns of SPECT in autism and Attention Deficit Hyperactivity Disorder (ADHD).
Autism: Autism is a developmental disorder of an early onset characterized by deficits in verbal and nonverbal language, social skills, cognitive ability and an abnormal behavior [11]. Some SPECT studies in young children using 99m-Tc HMPAO revealed abnormal rCBF in frontal and temporal cortices [10, 11]. Figure 2a is a SPECT brain scan of a 5-year-old boy with developmental delay and autism.
Attention deficit hyperactivity disorder (ADHD) is a developmental disorder characterized by a neurobehavioral syndrome with an onset in childhood. 99mTc HMPAO brain SPECT findings at rest and during intellectual stress in children and adolescents revealed decreased perfusion in the prefrontal cortex with intellectual stress [12]. Figure 2b is a SPECT brain scan of a 4 year old intellectually stressed child diagnosed with ADHD.
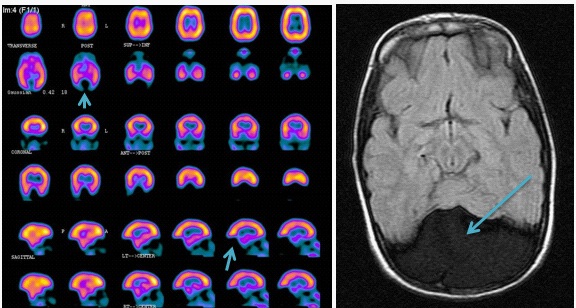
Brain death
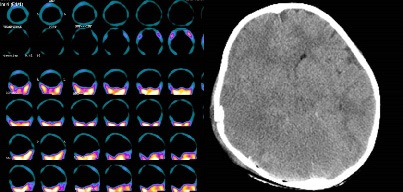
The diagnosis of brain death is based on clinical and laboratory tests including EEG [13,14]. When these tests are inconclusive, SPECT brain scan has recomended to confirm the clinically suspected brain death [15,22]. In addition it has been used in cases of organ donation when family members are welling to document the absent flow [23].
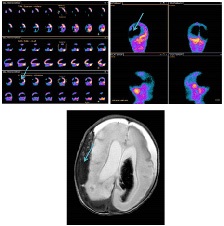
Figure 5 is a SPECT scan and a selected transaxial CT image of a patient with clinical brain death secondary to head trauma and the scan performed as a confirmatory test.
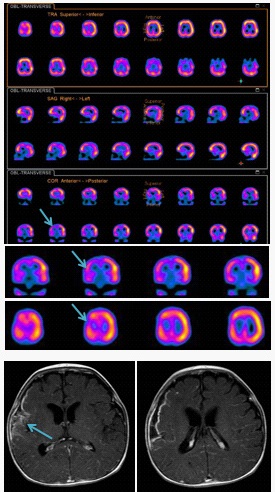
Mitochondrial disease
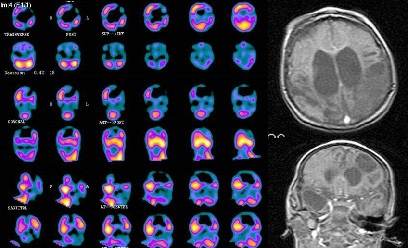
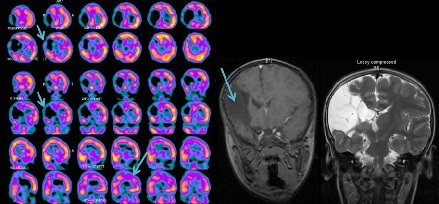
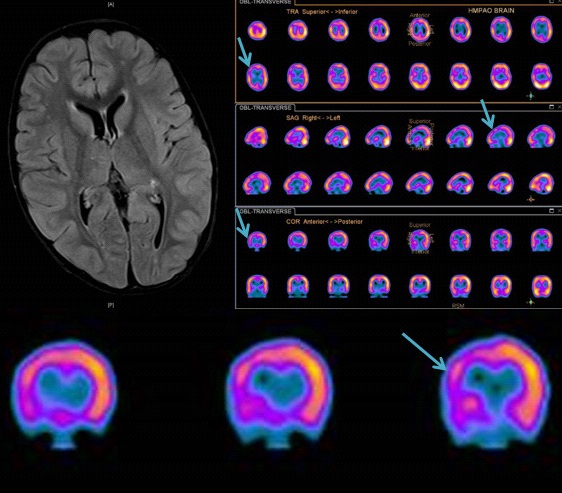
Mitochondrial disease is a multiorgan system disorder and the Central Nervous System (CNS) being the second most commonly affected [24]. The most pertinent CNS abnormalities in children with mitochondrial disorder on imaging include white and grey matter lesions, stroke-like lesions, brain and optic nerve atrophy, and calcifications [25]. Some of these lesions may remain without symptoms while others may present with stoke like symptoms or autism like symptoms. Different brain imaging modalities are used in the work up of those patients including CT, MRI, PET and SPECT scan. Because of daily availability, some of these techniques are more useful than others. SPECT brain scan is used to assess changes in rCBF caused by lesions seen on anatomic imaging in first place and to understand the pathophysiology of this disorder hence as mentioned before changes in perfusion are paralleled with changes in metabolism and neuronal activity. Figure 6 is a SPECT scan and selected MRI images of a patient with mitochondrial disease of the brain.
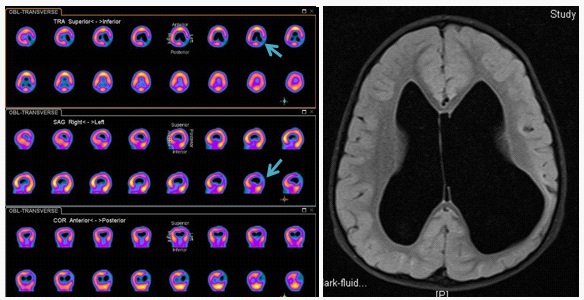
Vascular disorders: Moyamoya disease
Moyamoya Disease (MMD) is a vascular occlusive disease and was firstly described by T. K. Shimizu in 1957 as a “bilateral hypoplasia of internal carotid arteries” [26].
MR angiography and CT angiography are the imaging modalities currently used to assess the spectrum of vascular changes in moyamoya disease [27].
SPECT brain scan was used to assess cerebral hemodynamics in children with Moyamoya Disease [28] and to demonstrate the extent of the impaired rCBF in ischemic areas [29]. Figure 7: SPECT and MRI images of a 10 year-old boy with left sided hemiplegia due to MMD.
Brain inflammation and infections
Encephalitis refers to a diffuse brain parenchymal inflammation mainly due to viral infections. Meningitis is an inflammation of meninges surrounding both brain and spinal cord. It can be caused by viral, bacterial and fungal infections. Symptoms include headache, fever, confusion, drowsiness and fatigue, and in some cases seizures or convulsions, hallucinations, stroke, hemorrhage and memory problems may occur [30].
In acute viral encephalitis SPECT scan shows increased uptake in affected area which will be normalized or shows decreased uptake in follow up study [31].
Discussion
Changes in brain function can be assessed by brain perfusion studies hence flow and metabolism are paralleled process in most brain disorders with the exception of brain tumors [1]. MRI is currently the method of choice to assess rCBF by use of Arterial Spin-Labeling (ASL) and being noninvasive and with no radiation hazard [32] which requires a specialized center and expertise. 99m-Tc HMPAO or ECD SPECT can be used to measure regional cerebral perfusion [33] and the procedure can be performed in any nuclear department. M Gervil et al [34] in a group 27 children with neurological disorders and investigated by MRI and EEG they found that SPECT brain scan added important information to 21 patients and directly led to a change in diagnosis and better assessment of the prognosis in 4 of them. They concluded that SPECT is an important imaging modality in children with brain disorders of a partially or completely unknown etiology.
Conclusion
Although anatomic cross sectional imaging give details of neurological structural changes, SPECT perfusion mirrors indirectly both metabolic and neuronal activity changes. Therefore, accurate interpretation of SPECT perfusion will consolidate its role as part of the diagnostic protocol and used when the findings of other imaging modalities do not explain the symptoms or fail partially or completely in determining the etiology of brain disorders in pediatric patients.
References
- Raichle ME. Behind the scenes of functional brain imaging: A historical and physiological perspective. Proc Natl Acad Sci USA. 1998; 95: 765–772.
- Duncan AF, Caprihan A, Montague EQ, Lowe J, Schrader R, et al. Regional Cerebral Blood Flow in Children From 3 to 5 Months of Age AJNR Am J Neuroradiol. 2014; 35: 593-598.
- Camargo EE. Brain SPECT in neurology and psychiatry. J Nucl Med. 2001; 42: 611-623.
- Donohoe KJ(Chair), Agrawal G, Frey KA, et al. SNM Practice Guideline for Brain Death Scintigraphy . Journal Of Nuclear Medicine Technology. 2012; 40: 198-203.
- Matsuda H, Higashi S, Kinuya K, et al. SPECT evaluation of brain perfusion reserve by the acetazolamide test using Tc 99m HMPAO. Clin Nucl Med. 1991; 16: 572 579.
- Holman BL, Zimmerman RE, Johnson KA, et al. Computer assisted superimposition of magnetic resonance and high resolution technetium 99m HMPAO and thallium 201 SPECT images of the brain. J Nucl Med. 1991; 32: 1478 1484.
- Takahashi T, Shirane R, Sato S, Yoshimoto T. Developmental Changes of Cerebral Blood Flow and Oxygen Metabolism in Children AJNR Am J Neuroradiol. 1999; 20: 917-922.
- Sood S, Chugani HT. Functional neuroimaging in the preoperative evaluation of children with drug-resistant epilepsy. Childs Nerv Syst. 2006; 22: 810-820.
- Goffin K, Dedeurwaerdere S, Van Laere K, Van Paesschen W. Neuronuclear assessment of patients with epilepsy. Semin Nucl Med. 2008; 38: 227-239.
- Fisher RS, Cross JH, French JA, et al. Operational classification of seizure types by the International League Against Epilepsy. Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017; 58: 522-530.
- Jackson GD, Kuzniecky RI. Chapter 79. Structural Neuroimaging. In: Engel J, Pedley TA, eds. Epilepsy: A Comprehensive Textbook. 2 ed. Philadelphia PA: Wolters Kluwer/Lippincott Williams & Wilkins. 2008.
- http://www.nlm.nih.gov/medlineplus/ency/article/003200. html
- George MS, Costa DC, Kouris K, Ring HA, Ell PJ. Cerebral Blood Flow Abnormalities in Adults With Infantile Autism. J Ner Ment Dis. 1992; 180: 413-417.
- Mountz JM, Tolbert LC, Liii DW, Katholi CR, Liu HG. Functional Deficits in Autistic Disorder: Characterization by Technetium99m-HMPAO and SPECT. J NucIMed. 1995; 36: 1156-1162.
- Amen DG, Carmichael BA. High-resolution brain SPECT imaging in ADHD. Ann Clin Psychiatry. 1997; 9: 81-86.
- Flowers WM Jr, Patel BR. Accuracy of clinical evaluation in the determination of brain death. South Med J. 2000; 93: 203-206.
- Heran MK, Heran NS, Shemie SD. A review of ancillary tests in evaluating brain death. Can J Neurol Sci. 2008; 35: 409-419.
- Al-Shammri S, Al-Feeli M. Confirmation of brain death using brain radionuclide perfusion imaging technique. Med Princ Pract. 2004; 13: 267-272.
- Conrad GR, Sinha P. Scintigraphy as a confirmatory test of brain death. Semin Nucl Med. 2003; 33: 312-323.
- Harding JW, Chatterton BE. Outcomes of patients referred for confirmation of brain death by 99mTc-exametazime scintigraphy. Intensive Care Med. 2003; 29: 539-543.
- Lu G, Shih WJ, Ryo UY. Findings on Tc-99m HMPAO brain imaging in brain death. Clin Nucl Med. 1996; 21: 891-893.
- Munari M, Zucchetta P, Carollo C, et al. Confirmatory tests in the diagnosis of brain death: comparison between SPECT and contrast angiography. Crit Care Med. 2005; 33: 2068-2073.
- Okuyaz C, Gucuyener K, Karabacak NI, et al. Tc-99m-HMPAO SPECT in the diagnosis of brain death in children. Pediatr Int. 2004; 46: 711-714.
- Spieth M, Abella E, Sutter C, et al. Importance of the lateral view in the evaluation of suspected brain death. Clin Nucl Med. 1995; 20: 965-968.
- Wijdicks EF, Varelas PN, Gronseth GS, et al. Evidence-based guideline update: determining brain death in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2010; 74: 1911-1918.
- Harding JW, Chatterton BE. Outcomes of patients referred for confirmation of brain death by 99mTc-exametazime scintigraphy. Intensive Care Med. 2003; 29: 539-543.
- Gorman GS, Chinnery PF, DiMauro S, et al. Mitochondrial diseases. Nat Rev Dis Primers 2016; 2: 16080.
- Josef Finsterer and Sinda Zarrouk-Mahjoub. Cerebral imaging in paediatric mitochondrial disorders. Neuroradiol J. 2018; 31: 596-608.
- Takeuchi K, Shimizu K. Hypoplasia of the bilateral internal carotid arteries. Brain Nerve. 1957; 9: 37-43.
- Tarasów E, Kułakowska A, Łukasiewicz A, Kapica-Topczewska K, Korneluk-Sadzyńska A, et al. Moyamoya disease: Diagnostic imaging. Pol J Radiol. 2011; 76: 73-79.
- Nakagawara JSN, Nakamura H, et al. Assessment of cerebral hemodynamics in childhood moyamoya disease using a quantitative and a semi quantitative IMP-SPECT study. Ann Nucl Med. 2004; 18: 323-331.
- B.Volkan-Salancia E. Lay Ergüna Ç. Genc SelbD. YalnizoğlubG. Turanlib. The role of brain perfusion SPECT in moyamoya disease. Revista Española de Medicina Nuclear e Imagen Molecular. 2012; 31: 216-221.
- Millichap JJ, Epstein LG. Emerging subspecialties in neurology: neuroinfectious diseases. Neurology. 2009; 73: e14-15.
- Kao CH, Wang SJ, Mak SC, Shian WJ, Chi CS. Viral Encephalitis in Children: Detection with Technetium-99m HMPAO Brain Single-Photon Emission CT and Its Value in Prediction of Outcome. AJf’IR Am J f’leuroradio. 1994; 15: 1369-1373.
- Detre JA, Wang J, Wang Z, et al. Arterial spin-labeled perfusion MRI in basic and clinical neuroscience. Curr Opin Neurol. 2009; 22: 348-355.
- Kapucu OL, Nobili F, Varrone A, Booij J, Vander Borght T, Nagren K, et al. EANM procedure guideline for brain perfusion SPECT using 99mTc-labelled radiopharmaceuticals, version 2. Eur J Nucl Med Mol Imaging. 2009; 36: 2093-102.
- Gervil M, Andersen AR, Skriver EB, Lauritzen MJ, Knudsen FU. Clinical value of SPECT scanning in children with neurological disorders. Ugeskr Laeger. 1998; 160: 6965-6971.