
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Weight-lifter training causing pectoral neuropathy
Elena Merli1; Rita Rinaldi2; Maria Alessandria3 ; Roberto D’Alessandro4; Roberto D’Angelo2*
1IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy.
2 IRCCS Istituto delle Scienze Neurologiche di Bologna, Clinica Neurologica Rete Metropolitana, Bologna, Italy
3 ASL Lecce, DSS Martano, Lecce, Italy.
4 IRCCS Istituto delle Scienze Neurologiche di Bologna, Neuroepidemiology Unit, Bologna, Italy.
*Corresponding Author : Roberto D’Angelo
IRCCS Istituto delle Scienze Neurologiche di Bologna,
Clinica Neurologica Rete Neurologica Metropolitana,
Policlinico Sant’Orsola- Malpighi, Bologna, Building
2, Via Albertoni, 15 - 40138 Bologna, Italy.
Email: roberto.dangelo@aosp.bo.it
Received : Mar 27, 2021
Accepted : Apr 21, 2021
Published : Apr 23, 2021
Archived : www.jcimcr.org
Copyright : © D’Angelo R (2021).
Abstract
We report two weightlifters, presenting with progressive atrophy and weakness of the medial portion of pectoralis major muscle. We discuss possible differential diagnoses and propose a clinical and neurophysiological approach. Our cases highlight that the syndrome may be unilateral or bilateral, probably due to anatomical susceptibility and hyper-training. We review this rare syndrome and promote its awareness and full diagnostic assessment, aiming to its prompt recognition in weightlifters.
Keywords: Pectoral nerve; Pectoralis major muscle; Entrapment neuropathy; Nerve conduction study; weight-lifting.
Abbreviations: CK: Creatine Kinase; NCS: Nerve Conduction Study; EMG: Needle Electromyography Study; LPN: Lateral Pectoral Nerve; MPN: Medial Pectoral Nerve.
Citation: Merli E, Rinaldi R, Alessandria M, D’Alessandro R, D’angelo R. Weight-lifter training causing pectoral neuropathy. J Clin Images Med Case Rep. 2021; 2(2): 1065.
Introduction
Nerve injury is a rare complication of weight-lifting training and high-intensity upper limb exercise, caused by stretch injury or intramuscular compression of the nerve [1]. Isolated long thoracic, suprascapular and musculocutaneous nerve lesions have been reported [1]. In this scenario, also anectodal reports of pectoral nerve entrapment exist [2,3].
Nevertheless, pectoral neuropathy is most frequently described after acute compressions due to seatbelts in car accident injuries or after intraoperative lesions in chest and plastic surgery [3,4].
We report two patients presenting with pectoral muscle atrophy after intensive weight- lifting. We present neurophysiological assessment and discuss possible aetiology of unilateral or bilateral medial pectoral neuropathy.
Case series
Patient 1 is a 33 year-old man, practicing intensive body building training for many years, who complained progressive weakness and wasting of the left pectoral muscle since three months. Clinical examination showed isolated atrophy of the sternal portion of the left pectoralis major muscle, with sparing of the clavicular portion.
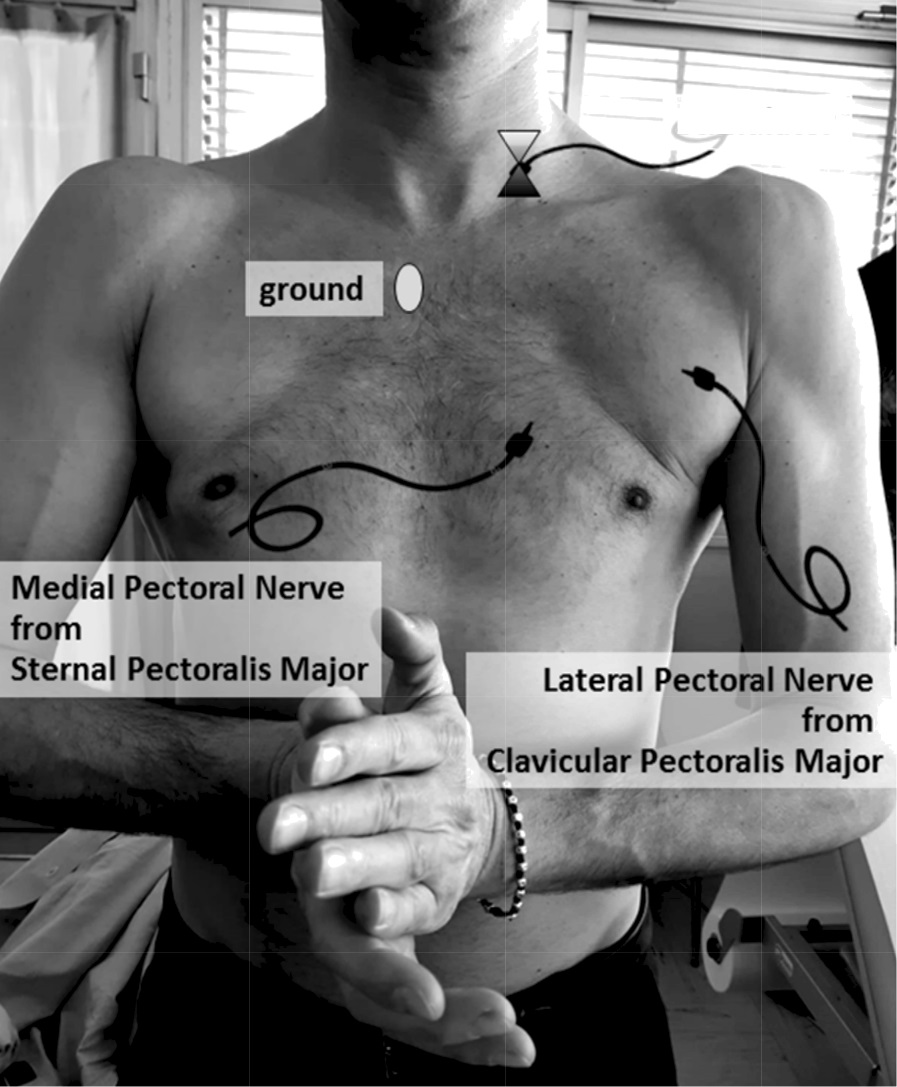
Patient 2 is a 46 year-old man, exercising regularly 4 times/ week at the gym, who presented with wasting of the sternal portion of both pectoral muscles, prevalent on the left. Clinical examination revealed isolated weakness and atrophy of bilateral sternal portions of pectoral muscles (Figure 1).
Pain was not referred by both patients.
On interrogation, they denied family history for neuromuscular diseases or use of anabolic steroids. An extended neuro logical examination excluded any weakness or atrophy of other muscles of anterior or posterior chest, of shoulders and arms. Muscular pain to compression, fasciculations or sensory signs were not elicited.
Creatine Kinase (CK) was mildly elevated while other laboratory findings and cervical spine MRI were unremarkable in both patients.
In order to exclude a sub-clinical broader muscle and nerve involvement, Nerve Conduction Study (NCS) and needle Electromyography Study (EMG) were performed. NCS with superficial electrodes was used to examine the upper limbs, while Lateral and Medical Pectoral Nerves (LPN and MPN) were bilaterally investigated by needle recording (Figure 1), according to Nacarkucuk et Ertekin [5].
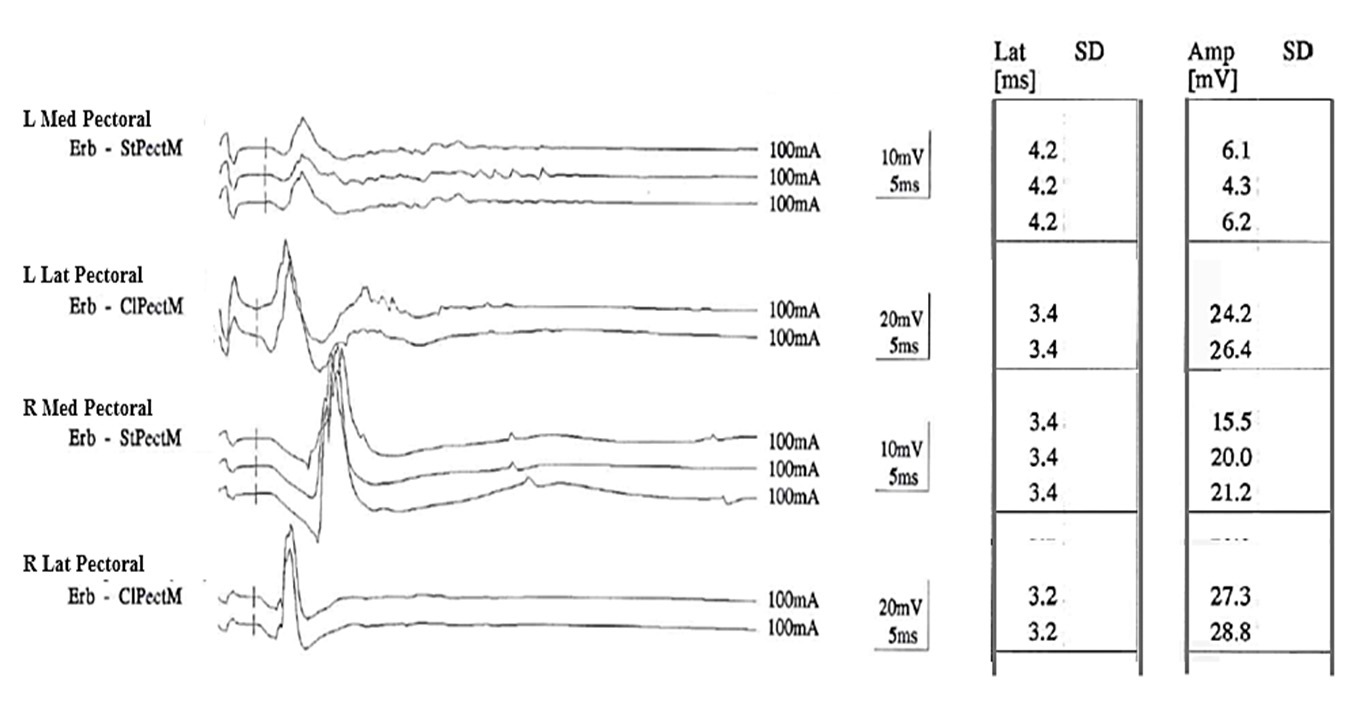
NCS of Patient 1 (Figure 2) showed slightly prolonged motor latency and reduced amplitude of motor potential of left MPN, while all other nerves examined, including LPN, were normal, suggesting a lesion of left MPN. NCS of Patient 2 showed similar but bilateral findings, concluding for a bilateral MPN neuropathy.
EMG of sternal portion of pectoralis major revealed augmented amplitude and duration of motor unit potentials, reduced interferential pattern and absence of spontaneous activity, unilaterally in Patient 1 and bilaterally in Patient 2. Clavicular portion of pectoralis major and shoulder and arm muscles (deltoid, biceps and triceps brachii, first dorsal interosseus) examined bilaterally were normal.
A diagnosis of medial pectoral entrapment neuropathy unilateral in patient 1 and bilateral in patient 2 was established.
Discussion
Surgical and postmortem studies [3,4] provide anatomical explanation for medial pectoral entrapment neuropathy: pectoralis major muscle is composed by an inferior sternal portion and a superior clavicular portion with different innervations. Motor fibres innervating the sternal portion originate from the 8th cervical and 1st thoracic ventral radicular branches, contribute to the medial cord of brachial plexus and compose MPN. This passes between axillary artery and vein and joins a branch of the LPN. Subsequently, it splits in some terminal branches. Some of these enter the deep surface of the minor pectoral muscle to supply it, while others pass below the inferior border of minor pectoral muscle and enter into the sternal portion of major pectoral muscle. Motor fibres supplying the clavicular portion derive from the 5th to 7th cervical branches, participate to the anterior division of the upper and middle trunks or directly to lateral cord and finally compose LPN. It crosses anteriorly the axillary artery and vein, sends a branch to the MPN and enters the clavipectoral fascia to terminate in clavicular major pectoral muscle.
Notably, both terminal nerves have potential sites of entrapment, so lesions due to compression by thickened hypertrophied connective and muscle tissues or microtraumas during repetitive exercises may develop [3]. In particular LPN may be compressed between clavipectoral fascia and subclavius muscle [3], while MPN may be compressed passing directly through the pectoralis minor muscle [6], as probably happened in our two patients.
From a clinical point of view, we highlight the possible occurrence of weakness and atrophy in pectoral muscles in men who train regularly. Generally, the acute onset and the presence of intense localized pain, swelling, ecchymoses or a palpable abnormality suit for a tendon or muscle rupture [7]. On the contrary, the progressive onset of symptoms is evocative for a neurological cause. Possible diagnoses are focal disorders (radiculopathy, brachial plexus neuropathy, isolated pectoral neuropathy) or neuromuscular diseases (motor neuron disease or myopathy) [1,6,7]. The distribution of pain and sensory symptoms, along with the localization of weakness, atrophy or other signs of neuromuscular involvement (i.e fasciculations) may direct the suspicion. Further exams should then be performed, starting from laboratory tests (including CK), cervical spine MRI, NCS and EMG, to clarify the diagnosis, which is crucial for both prognosis and therapy.
MPN entrapment neuropathy is a non progressive, potentially reversible disorder after training discontinuation.
In non-reversible cases after rest, a surgical therapeutic option exists, consisting in epineurotomy in order to decompress the nerve. Previous reports on very small samples of patients showed encouraging results [3].
Conclusions
The reported cases confirm the occurrence of medial pectoral entrapment neuropathy in sports men practicing regularly high-intensity upper limb exercise. We promote the awareness of this syndrome and its recognition particularly in weightlifters and we suggest an NCS/EMG protocol (Figure 1 and 2) to confirm the diagnosis.
References
- Hainline BW. Peripheral Nerve Injury in Sports. Continuum (Minneap Minn). 2014; 20: 1605–1628.
- Bird SJ, Brown MJ. Acute focal neuropathy in male weigth lifters. Muscle Nerve. 1996; 19: 897-899.
- Gardetto A, Thaler C, Kiechl S, Maurer H, Piza-Katzer H. Isolated compression of the pectoral nerve resulting in atrophy of the mayor pectoral muscle. Muscle Nerve. 2003; 28: 760-763.
- Hoffman GW, Elliott LF. The anatomy of the pectoral nerves and its significance to the general and plastic surgeon. Ann Surg. 1987; 205: 504 –507.
- Nacarkucuk E, Ertekin C. Lateral pectoral nerve conduction. Intern J Neuroscience 2004; 114: 451-458.
- Rossi F, Triggs WJ, Gonzalez R, Shafer SJ. Bilateral medial pectoral neuropathy in a weight lifter. Muscle Nerve. 1999; 22: 1597- 1599.
- Kerr ZY, Collins CL, Comstock RD. Epidemiology of weight training-related injuries presenting to United States emergency departments, 1990 to 2007. Am J Sports Med 2010; 38: 765-771.