
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Concomitant chromosome 5q-deletion and JAK2V617F mutation present with myelodysplastic and myeloproliferative overlap features
Laura Miotke1; Jay Patel2; Josef T Prchal3; Srinivas K Tantravahi1*
1Department of Internal Medicine, University of Utah, Salt Lake City, UT, USA.
2 Department of Pathology ARUP Laboratories, University of Utah, Salt Lake City, UT, USA.
3 Division of Hematology and Hematologic Malignancies, Huntsman Cancer Hospital, University of Utah, Salt Lake City, UT, USA.
*Corresponding Author : Srinivas K Tantravahi
Huntsman Cancer Institute, The University of Utah,
Salt Lake City, USA-84112.
Email: Srinivas.tantravahi@hci.utah.edu
Received : Mar 27, 2021
Accepted : Apr 22, 2021
Published : Apr 26, 2021
Archived : www.jcimcr.org
Copyright : © Tantravahi SK (2021).
Citation: Miotke L, Patel J, Prchal JT, Tantravahi SK. Concomitant chromosome 5q-deletion and JAK2V617F mutation present with myelodysplastic and myeloproliferative overlap features. J Clin Images Med Case Rep. 2021; 2(2): 1068.
Introduction
Myelodysplastic Syndrome (MDS) with an isolated deletion of chromosome 5q [del(5q)] is a relatively rare MDS variant (5%) characterized by a moderate to severe anemia and normal or elevated platelet count with modest neutropenia [1-3]. These latter features, in addition to its excellent response to lenalidomide, are likely what contribute for its favorable prognosis [3-5]. The somatic gain of function mutation in JAK2 V617F is a driving mutation in Myeloproliferative Neoplasms (MPN), occurring in 97% of polycythemia vera (PV), 50-60% of essential thrombocytosis (ET) and primary myelofibrosis (PMF) [6]. This mutation results in constitutive activation of the JAK-STAT signaling pathway leading to increased proliferation and hypersensitivity to cytokines erythropoietin, IL-3, thrombopoietin, and GCSF. An allelic burden of JAK2 V617F mutation correlates with an increased risk of thrombosis and hemorrhage, as well as secondary fibrosis in MPN patients [7]. Compared to MPNs, JAK2 mutations are infrequent in MDS, occurring in less than 5% of the cases. This frequency is mirrored in the del(5q) subtype [8,9]. Concomitant presence of JAK2 V617F and del(5q) has been reported in the literature, although not much is known about how the prognosis of this combination differs from an isolated del(5q); and in particular with the risk of transformation to Acute Myeloid Leukemia (AML) and response to lenalidomide therapy. While classified as an MDS subset, patients with this combination exhibit specific clinical and pathologic features characteristic of both MDS and MPN. There have been reports that these patients present with a more proliferative bone marrow and retain morphologic features of MPN even after transformation to AML [10,11]. Here we describe two patients with a concomitant JAK2 V617F mutation and del5(q), both presenting with severe macrocytic anemia, marked thrombocytosis and characteristic bone marrow morphology.
Case description
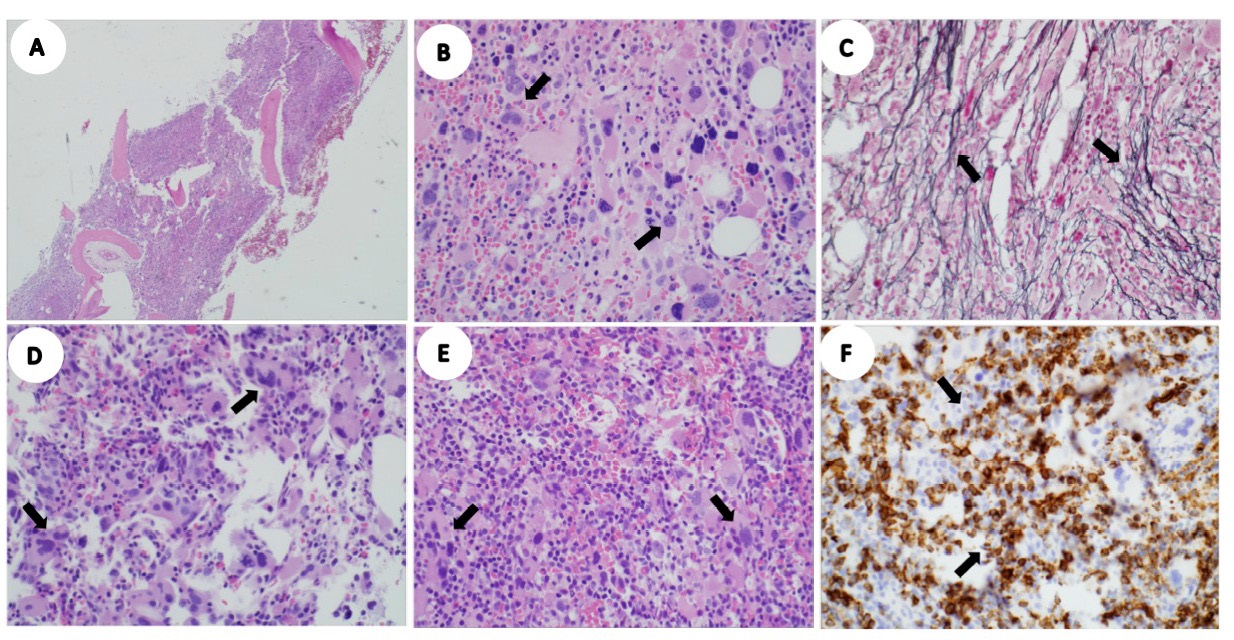
The first patient is a 49-year-old woman who presented with exertional shortness of breath and exercise intolerance. Complete Blood Count (CBC) showed severe anemia, hemoglobin of 76 g/L and marked thrombocytosis, platelet count of 673 X 109 /L (Table 1). Physical exam revelated marked pallor without lymphadenopathy or splenomegaly. Marrow biopsy was hypercellular (Figure 1A) with a myeloid predominance, no increase in myeloblasts and prominent clustering of atypical hypolobated megakaryocytes with hyperchromatic nuclei (Figure 1B). Reticulin stain showed mild to focally moderate reticulin fibrosis, MF grade 1-2/3 (Figure 1C), without any collagen fibrosis. Myeloid mutation panel by Next-Generation Sequencing (NGS) revealed one tier 1 mutation, JAK2 V617F , with a variant frequency of 33%. Marrow karyotype showed del5(q13q33) in 20/20 cells. Based on the presence of del5(q), she was treated with lenalidomide 10 mg daily and was transfused with red cells. After approximately six weeks of treatment, she developed severe pancytopenia and a delayed hemolytic transfusion reaction mediated by anti-E and anti-Lu9(a) antibodies. Subsequently, she was unable to tolerate lenalidomide, despite a dose reduction, due to grade 3- 4 neutropenia. She elected to discontinue lenalidomide and was later switched to intravenous azacitidine 75 mg/ m2 for five consecutive days, every 28 days. To date, patient received 6 cycles of azacitidine with no hemoglobin response and continues to require red cell transfusions.
Table 1: Summary of pertinent laboratory studies.
|
Patient 1 |
Patient 2 (at the time of diagnosis) |
Patient 2 (at progression to AML) |
WBC count |
6.8X109/L |
5.1X109/L |
2.5X109/L |
Hemoglobin |
76 g/L |
81g/L |
89g/L |
Platelet |
673X109/L |
887X109/L |
262X109/L |
Peripheral blood blasts% |
None |
None |
14% |
Bone marrow cellularity |
90% |
60% |
80% |
Bone marrow blasts % on morphology |
2.5% |
<1% |
65% |
Karyotype |
46,XX,del(5)(q13q33)[20] |
46,XX,del(5)(q31q35)[18]/46,XX[2] |
46,XX,del(5)(q31q35)[18]/48,sl,+8[1]/46,XX[1] |
Somatic mutations on myeloid NGS panel (VAF%) |
1. JAK2 c.1849G>T, p.Val617Phe (NM_004972.3) |
1. JAK2 c.1849G>T, p.Val617Phe (NM_004972.3) 2. DNMT3A c.2579G>A, p.Trp860* (NM_175629.2) 3. ASXL1 c.1720-1G>A, p.? (NM_015338.5) 5. KRAS c.351A>T, p.Lys117Asn (NM_004985.4) 6. GATA2 c.1075T>G, p.Leu359Val (NM_001145661.1)
|
1. JAK2 c.1849G>T, p.Val617Phe (NM_004972.3) 2. DNMT3A c.2579G>A, p.Trp860* (NM_175629.2) 3. ASXL1 c.1720-1G>A, p.? (NM_015338.5) 4. BCOR c.3254dup, p.Asn1086fs (NM_001123385.1) 5. KRAS c.351A>T, p.Lys117Asn (NM_004985.4) 6. GATA2 c.1075T>G, p.Leu359Val (NM_001145661.1) 7. ETV6 c.428_429dup, p.Pro144fs (NM_001987.4) |
The second patient, a 72- year-old woman, presented with severe fatigue, 25lbs of unintentional weight loss over one year and aquagenic pruritus. CBC at initial presentation showed similar findings to Patient 1 with a normal white blood cell count, severe anemia, and marked thrombocytosis (Table 1). Physical exam was notable for splenomegaly measuring 8 cm from the left costal margin in the midclavicular line. Marrow examination revealed hypercellular marrow with increased myeloblasts (10-15%) and atypical hypolobated megakaryocytes in clusters (Figure 1D). Karyotype showed an isolated del5(q31q35) in 18/20 (90%) cells. The myeloid NGS panel showed multiple tier 1 mutations in JAK2, GATA2, DNMT3A, ASXL1, BCOR, and KRAS (Table 1). Based on increased blast percentage, treatment with azacitidine was recommended but the patient declined intravenous therapy. Oral lenalidomide was recommended for the treatment of anemia. After three months of oral lenalidomide treatment, hemoglobin and platelet counts normalized and marrow examination after 6 months of lenalidomide treatment showed del5(q) in 3/20 (15%) cells. Anemia response was maintained for approximately one year, at which point patient developed progressive anemia and thrombocytopenia. Marrow examination continued to show clusters of atypical megakaryocytes (Figure 1E) and 60% myeloblasts on CD34 immunostaining indicating progression to AML (Figure 1F). No substantial changes in JAK2 V617F allele burden was observed on treatment with lenalidomide or at progression to AML (Table 1). She received remission induction with liposomal daunorubicin and cytarabine [12]. A complete response was observed on follow up marrow examination and she subsequently received consolidation therapy with liposomal formulation of cytarabine and daunorubicin (Vyxeos). An allogenic stem cell transplant was recommended to the patient; however, she declined and remains in remission after one year since achieving a CR.
Discussion
As previously reported in patients with a concomitant del(5q) and JAK2 V617F mutation, the hallmark of our patients’ presentations include anemia and marked thrombocytosis [10]. A majority of patients are also transfusion dependent [10,13,14]. While this appears similar to MPNs, the transfusion-dependent anemia and thrombocytosis does not typically respond to erythropoietin and hydroxyurea respectively [14-16]. In some cases with a del (5q) and JAK2 V617F mutation, platelet and leukocyte counts did normalize with a regimen of interferon-alpha, aspirin and hydroxyurea, but this did not improve the anemia [10,13]. This behavior, as well as the response to lenalidomide, is more similar to an MDS-type clinical course. In most case reports, treatment with lenalidomide obliterates all cellular clones with del(5q) and in some cases reduction in JAK2 V617F positive clone was observed [13-16]. For example, a complete molecular response occurred in one patient with undetectable JAK2 V617F mutation by quantitative real time polymerase reaction after 9 months of lenalidomide treatment compared to baseline JAK2 V617F allele burden of 26.28% [14]. In another case report, JAK2 V617F allele burden reduced from 18.472% from baseline to 0.018% after 6 months of lenalidomide treatment [15]. Transient clinical response to single agent lenalidomide was also reported in one patient who presented with transformation to AML with history of previously untreated MDS with del(5q) and JAK2 V617F mutation [17]. Interestingly, this patient was JAK2 V617F positive at transformation to AML similar to our patient 2 [17]. As previously reported grade 3/4 neutropenia is common with lenalidomide treatment, as experienced in patient 1 [18]. The marrow of our patients did not demonstrate overt morphologic features of dysplasia, but showed numerous hypolobated megakaryocytes more consistent with MPN. These MPN-like features were preserved in transformation to AML in patient 2, similar to prior reports [11]. A recent analysis of 5q deletion patients showed that the additional somatic mutations with highest frequency of were SF3B1, DNMT3A, TP53, TET2, CSNK1A1 and ASXL1, as well as JAK2 genes. Mutations occurred commonly as singular mutations (43%) or with one additional somatic mutation (23%) and it was rare to have three or more somatic mutations such as in patient 2. CSNK1A1 and SF3B1 were the only two mutations found to be significantly associated with each other. The presence of an SF3B1, TP53, or RUNX1 mutation were each suggestive of a higher likelihood of transformation to AML and worse prognosis [9]. Whether the prognosis and transformation to AML differs in patients with concomitant 5q deletion and JAK2 mutation is unknown. Less than 10% of patients with an isolated deletion 5q transform to AML, although this occurred in one of our two patients. However, there is a paucity of literature describing the concomitant presence of these two hematological entities. Significant focal myelofibrosis (2/3) was demonstrated in patient 1 as well (Figure 1B), which is rarely seen in 5q syndrome but has been reported before in 5q syndrome with a JAK2 mutation [19]. This indicates the need for longer follow-up data and greater study numbers to assess more accurately leukemic transformation rates and predict prognosis in this population. Based on the mixed clinical picture, response to treatment and possibly distinct rates of transformation to AML, perhaps del(5q) patients with concomitant JAK2V617F mutation should be categorized as myelodysplastic/myeloproliferative neoplasms (MDS/MPN).
References
- Van den Berghe H, Cassiman JJ, David G, Fryns JP, Michaux JL, Sokal G. Distinct haematological disorder with deletion of long arm of no. 5 chromosome. Nature. 1974; 251: 437-438.
- Boultwood J, Pellagatti A, McKenzie AN, Wainscoat JS. Advances in the 5q- syndrome. Blood 2010; 116: 5803-5811.
- Patnaik MM, Lasho TL, Finke CM, et al. WHO-defined ‘myelodysplastic syndrome with isolated del(5q)’ in 88 consecutive patients: survival data, leukemic transformation rates and prevalence of JAK2, MPL and IDH mutations. Leukemia. 2010; 24: 1283-1289.
- Mallo M, Del Rey M, Ibanez M, et al. Response to lenalidomide in myelodysplastic syndromes with del(5q): Influence of cytogenetics and mutations. Br J Haematol. 2013; 162: 74-86.
- Talati C, Sallman D, List A. Lenalidomide: Myelodysplastic syndromes with del(5q) and beyond. Semin Hematol. 2017; 54: 159-166.
- Passamonti F, Maffioli M, Caramazza D, Cazzola M. Myeloproliferative neoplasms: from JAK2 mutations discovery to JAK2 inhibitor therapies. Oncotarget 2011; 2: 485-490.
- Kralovics R, Passamonti F, Buser AS, et al. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N Engl J Med. 2005; 352: 1779-1790.
- Haferlach T, Nagata Y, Grossmann V, et al. Landscape of genetic lesions in 944 patients with myelodysplastic syndromes. Leukemia. 2014; 28: 241-247.
- Meggendorfer M, Haferlach C, Kern W, Haferlach T. Molecular analysis of myelodysplastic syndrome with isolated deletion of the long arm of chromosome 5 reveals a specific spectrum of molecular mutations with prognostic impact: A study on 123 patients and 27 genes. Haematologica. 2017; 102: 1502-1510.
- Ingram W, Lea NC, Cervera J, et al. The JAK2 V617F mutation identifies a subgroup of MDS patients with isolated deletion 5q and a proliferative bone marrow. Leukemia. 2006; 20: 1319- 1321.
- Pich A, Godio L, Riera L, et al. Myelodysplastic syndrome with del (5q) and JAK2(V617F) mutation transformed to acute myeloid leukaemia with complex karyotype. Ann Hematol. 2016; 95: 525-527.
- Lancet JE, Uy GL, Cortes JE, et al. CPX-351 (cytarabine and daunorubicin) Liposome for Injection Versus Conventional Cytarabine Plus Daunorubicin in Older Patients With Newly Diagnosed Secondary Acute Myeloid Leukemia. J Clin Oncol. 2018; 36: 2684-2692.
- Hatzimichael E, Lagos K, Vassou A, Gougopoulou D, PapoudouBai A, Briasoulis E. Durable response to lenalidomide in a patient with myelodysplastic syndrome associated with isolated 5q deletion and JAK2 V617F mutation despite discontinuation of treatment. Mol Clin Oncol. 2016; 5: 23-26.
- Musto P, Simeon V, Guariglia R, et al. Myelodysplastic disorders carrying both isolated del(5q) and JAK2(V617F) mutation: concise review, with focus on lenalidomide therapy. Onco Targets Ther. 2014; 7: 1043-1050.
- Nomdedeu M, Maffioli M, Calvo X, et al. Efficacy of lenalidomide in a patient with myelodysplastic syndrome with isolated del(5q) and JAK2V617F mutation. Leuk Res. 2011; 35: 1276-1278.
- Vaccarino A, Dogliotti I, Marletto F, Demarchi A, Bazzan M. Diagnosis of del(5q) MDS, 14 Years after JAK-2 Positive PV Appearance: Complete Remission of both Diseases with Lenalidomide Monotherapy. Mediterr J Hematol Infect Dis. 2016; 8: e2016050.
- Mesa RA, Tefferi A, Li CY, Steensma DP. Hematologic and cytogenetic response to lenalidomide monotherapy in acute myeloid leukemia arising from JAK2(V617F) positive, del(5)(q13q33) myelodysplastic syndrome. Leukemia. 2006; 20: 2063-2064.
- List A, Dewald G, Bennett J, et al. Lenalidomide in the myelodysplastic syndrome with chromosome 5q deletion. N Engl J Med. 2006; 355: 1456-1465.
- Tremblay-LeMay R, Chang H. Concurrent JAK2 mutation and isolated del(5q) associated with marrow fibrosis and small hypo/ monolobated megakaryocytes. Blood. 2018; 132: 112.