
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Lateral sliding flap for one-step reconstruction of medium-sized eyelid defects
Dion Paridaens1,2
1The Rotterdam Eye Hospital, Oculoplastic & Orbital Service, Rotterdam, Netherlands.
2 Erasmus Medical Center, Department of Ophthalmology, Orbital Service, Rotterdam, Netherlands.
*Corresponding Author : Dion Paridaens
Oculoplastic & Orbital Service, The Rotterdam Eye
Hospital & Department of Ophthalmology, Erasmus
Medical Center, Dr Molenwaterplein 40, 3015 GD
Rotterdam, Netherlands.
Email: d.paridaens@oogziekenhuis.nl
Received : Mar 23, 2021
Accepted : Apr 22, 2021
Published : Apr 26, 2021
Archived : www.jcimcr.org
Copyright : © Paridaens D (2021).
Abstract
Background/purpose: To report the results of our clinical study on the efficacy of a ‘Lateral Sliding Flap’: A one-step technique for lower or upper eyelid reconstruction.
Methods: Retrospective analysis of a consecutive case series of patients treated with a ‘Lateral Sliding Flap’ following tumour removal by horizontal block excision. In this technique a (medium-sized) defect of up to 50% of the eyelid was reconstructed by disinsertion of the lateral canthus, medial advancement of the lateral (remaining) (full-thickness) eyelid and a laterally-based horizontal skin-muscle advancement flap, followed by canthal fixation. We recorded the operating time and evaluated the postoperative eyelid apposition, lid contour, complications and frequency and type of re-operation. The outcome was scored (according to four grades (excellent/good/fair/ poor) of lid apposition and contour.
Results: Seven consecutive patients, all treated by one oculoplastic surgeon in one year, were included. Six were female, one was male. Five had lower eyelid defects, two had upper eyelid defects of 40-50% of the horizontal width. The average age was 67,9 years, ranging from 52 to 85 years. The mean postoperative follow-up time was 31 months, ranging from 21-43 months. The average duration of the reconstruction was 31 minutes (ranging from 25 to 38 minutes). The outcome was excellent in 3 patients, good in 3 patients and fair in one patient. (Some) lash loss may be encountered. No complications such as flap ischemia of necrosis were noted. No re-operation was required.
Conclusion: The ‘Lateral Sliding Flap’ is an efficaceous, one-step technique for reconstruction of defects of up to 50% of the lower or upper eyelid. With the technique a normal eyelid margin is created at the level of the cornea for optimal visual function and comfort. Compared to Tenzel’s semicircular rotation flap, the ‘lateral sliding flap’ results in a shorter vertical scar and “Hidden” horizontal scars in the relaxed skin tension lines.
Keywords: Eyelid reconstruction; One-step; Lateral sliding flap.
Citation: Paridaens D. Lateral sliding flap for one-step reconstruction of medium-sized eyelid defects. J Clin Images Med Case Rep. 2021; 2(2): 1069.
Introduction
Eyelid reconstruction should be simple and efficaceous, and should also aim at acquiring both an optimal functional and cosmetic result. A one-step technique is preferred over a two step technique if the outcome is comparably good [1].
While primary closure (assisted with a lateral canthotomy) may be used for defects up to a horizontal width of 30% of the eyelid, other techniques are needed to close larger defects. A widely used single-step technique for horizontal defects up to 40-50% of the lower eyelid is Tenzel’s rotation flap [2]. In this technique a pentagonally shaped defect is closed with a semicircular skin/muscle flap from the area temporally of the lateral canthus. Although this technique nicely restores the eyelid margin at the level of the cornea, the resulting semicircular scar may (rarely) be cosmetically disturbing, as the incisional line does not follow the relaxed skin tension lines. The combination of a laterally-based skin-muscle and (full-thickness) horizontal sliding eyelid flap for lower lid reconstruction was reported in textbooks by Mustardé in 1980,[3] followed by Tyers and Collin in 1995 [4].
Here, we describe our (long-term) results of our patients treated with this technique for reconstruction of both lower lid and upper lid defects. To our knowledge, no other clinical evaluation study on this technique has been reported, while-to dateits use in the upper lid has not been described.
Methods
We performed a retrospective analysis of a consecutive case series of patients treated with eyelid reconstruction using a laterally-based horizontal sliding flap.
All patients had undergone frozen section controlled, radical tumour removal by ‘Horizontal Block’ excision prior to lid reconstruction. None of the patients was treated with pentagonal block excision. The defect size was measured with a pair of calipers, while approximating the wound edges with the use of forceps.
The defect was closed with a laterally-based horizontal skinmuscle and full-eyelidthickness sliding flap following disinsertion of the lateral canthus. The ‘lateral sliding’ flap includes the following steps (Figure 1):

1. Marking of the flap. With a marker-pen, a line is drawn in
a lateral direction starting from the inferior border of the
eyelid defect, following the relaxed skin tension line. This
line is extended laterally of the level of the outer canthus,
depending on the horizontal width of the eyelid defect.
A second line is drawn from the lateral canthus laterally
(‘Burke’s line’), parallel to the lower line, with a maximum
of about 2 cm, extending no further than the lateral brow.
2. Local anaesthesia. The lower eyelid and the lateral canthus are infiltrated with a mixture of xylocain 2% and
adrenalin 1:200.000 (about 3-4 cc). This infiltration was
also done in procedures under general anesthesia.
3. With a scalpel (no 15 blade), a full thickness cut in the
lower eyelid is made in the lower line up to the level of
the lateral canthus. The cut is extended laterally, following the marking, including the skin/muscle layer.
4. A second skin/muscle cut is made starting at the lateral
canthus towards lateral, according to the upper line.
5. The inferior limb of the lateral canthal tendon is cut with
a pair of straight (Steven’s) scissors.
6. The flap lateral of the lateral canthus is undermined below the muscle level up to the lateral base. Any bleeding
vessels are cauterized using bipolar cautery.
7. The laterally-based flap is advanced medially and sutured
to medial edge of the lower eyelid defect. The suturing
may consist of double-or single layer closure. For double
layer closure we use two intermittent vicryl 6.0 sutures
for the tarsus and two or three fast-absorbing vicryl 6.0 or
prolene 6.0 for the skin. For single layer closure of tarsus,
orbicularis muscle and skin, we use two or three intermittent prolene 6.0 or prolene 5.0 sutures [5].
8. Any redundant tissue at the eyelid margin, originating
from the previous canthal angle and interfering with an
optimal lid contour, can be shaved of the margin.
9. The inferior border of the lateral sliding flap is sutured in
two layers: The lower eyelid retractors are re-attached to
the lower part of the flap with two to three vicryl 6.0 sutures. The skin is closed at the end of the procedure.
10. The lateral canthus is reconstructed through fixation of
the flap to the intact superior limb of the lateral canthal
tendon and periosteum with a single buried vicryl 5.0 suture.
11. The subcutaneous musle layer of the flap is closed with
intermittent buried vicryl 5.0 sutures.
12. The skin of the flap (lower and upper border) is closed
with a running prolene 6.0 suture.
13. Steristrips are applied temporally of the lateral canthus
for vertical support and left in place for 5 days.
For upper eyelid reconstruction a similar lateral eyelid flap can be used. The height of the tarsus, i.e. 10 mm on average in the adult, should be indicative of the vertical dimension of the flap. The upper eyelid elevators are sutured back in place, as are the lower lid retractors in the lower eyelid (step 9, above).
Reconstruction was performed by creating a laterally-based horizontal advancement flap. disinsertion of the lateral canthus, medial advancement of the lateral (remaining) eyelid and a lateral skin-muscle flap, followed by canthal fixation. We recorded the operating time. Suture removal was performed at 5-7 days postoperatively, follow-up visits were planned at 3, 6, 9, 12 months and each following year) after surgery. We evaluated the postoperative eyelid apposition, lid contour, and complications (e.g. granuloma, infection, wound dehiscence, exposure keratopathy). The outcome was scored (according to four grades (excellent/good/fair/poor) of lid apposition and contour
Results
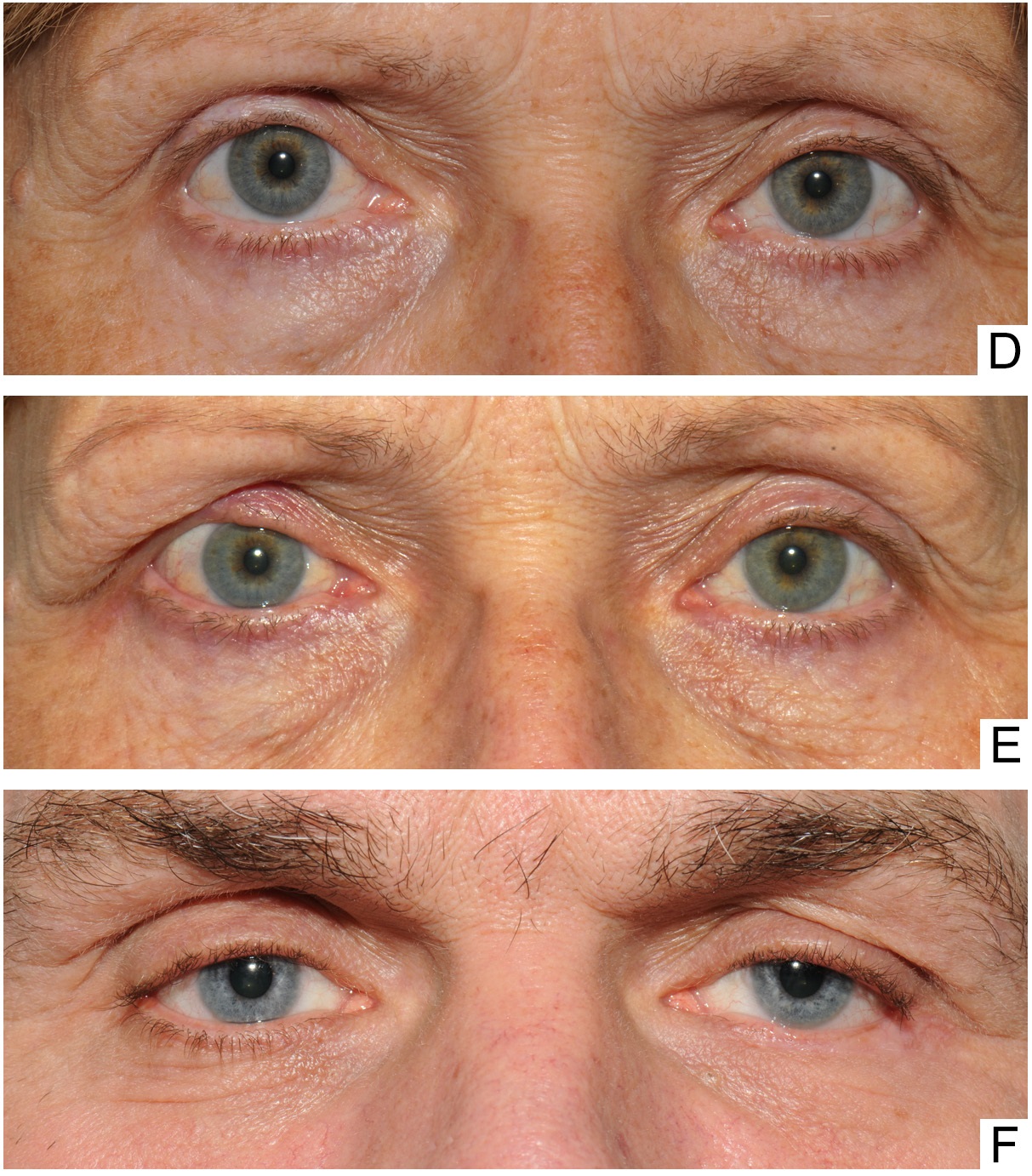
Seven consecutive patients, all treated by one oculoplastic surgeon (DP) in 2015, were included (Table 1). The average vertical defect size was 7.6 mm (range 6 to 12 mm). The average horizontal defect size was 11.6 mm (range 9 to 15 mm). The average duration of the reconstruction was 31 minutes (ranging from 25 to 38 minutes). Six patients were treated under general anesthesia, 1 under local anesthesia. The mean postoperative follow-up time was 19 months, ranging from 9 to 31 months. The outcome was excellent in 3 patients, good in 3 patients and fair in one patient. The apposition was good in all cases. The scars were well hidden in the natural, relaxed tension lines of the periocular skin (Figure 2). Patient 2 had some lash loss at the end of follow-up. Patient 3 had mild punctate corneal staining in the context of Meibomian gland dysfunction. In patient 7 we noted mild notching of the right upper eyelid with a pre-existent medial droop of the upper eyelid. No signs of tumour recurrence were noted during follow-up. No complications were noted. No re-operation was required.
Table 1: Clinical data of consecutive series of 7 patients who underwent lid reconstruction with the lateral sliding flap technique. LLL: left lower lid; RLL: right lower lid; RUL: right upper lid
Patient |
Gender |
Age (yrs) |
Location |
Defect width x |
Outcome at |
Follow-up |
1 |
F |
69 |
LLL |
11x6 |
Excellent |
21 |
2 |
F |
53 |
LLL |
13x7 |
Good |
37 |
3 |
F |
85 |
LLL |
9x9 |
Excellent |
29 |
4 |
F |
78 |
RLL |
12x6 |
Good |
36 |
5 |
M |
52 |
LLL |
15x6 |
Excellent |
25 |
6 |
F |
78 |
RUL |
12x12 |
Good |
43 |
7 |
F |
60 |
RUL |
9x7 |
Fair |
26 |
A. Marking of the flap. With a marker-pen, a line is drawn in a lateral direction starting from the inferior border of the eyelid defect, following the relaxed skin tension line. This line is extended laterally of the level of the outer canthus, depending on the horizontal width of the eyelid defect. A second line is drawn from the lateral canthus laterally (‘Burke’s line’), parallel to the lower line, with a maximum of about 2 cm, extending no further than the lateral brow.
B. With a scalpel (no 15 blade), a full thickness cut in the lower eyelid is made in the lower line up to the level of the lateral canthus.
C. The cut is extended laterally, following the marking, including the skin/muscle layer.
D. Another skin/muscle cut is made lateral of the outer canthus, in Burke’s line.
E. Following horizontal transection of the lowerlid retractor/ palpebral conjunctiva layer, the inferior limb of the lateral canthal tendon is cut with a pair of straight (Steven’s) scissors.
F. The flap lateral of the lateral canthus is undermined below the muscle level up to the lateral base. Any bleeding vessels are cauterized using bipolar cautery.
G. The laterally-based flap is advanced medially and sutured to the medial edge of the lower eyelid defect.
H. The lid margin can be closed with a double- or single layer closure. For double-layer closure we use two intermittent vicryl 6.0 sutures for the tarsus and two or three fast-absorbing vicryl 6.0 or prolene 6.0 for the skin. For single layer closure of tarsus, orbicularis muscle and skin, we use two or three intermittent prolene 6.0 or prolene 5.0 sutures, as we reported previously (Verhoekx et al. 2016).
I. Any redundant tissue at the eyelid margin, originating from the previous canthal angle and interfering with an optimal lid contour, can be shaved of the margin.
J. Following the suturing of the conjunctiva/lower retractors to the inferior border of the lateral eyelid flap with 2 to 3 vicryl 6.0 sutures, the lateral canthus is reconstructed through fixation of the flap to the intact superior limb of the lateral canthal tendon and periosteum with a single buried vicryl 5.0 suture.
K. The subcutaneous musle layer of the flap is closed with two intermittent buried vicryl 5.0 sutures.
L. The skin of the flap (lower and upper border) is closed with a running prolene 6.0 suture.
Discussion
Our study presents the long-term results of the firstly reported series of patients treated with a lateral sliding flap technique for one-step reconstruction of defects of up to 50% of both the lower or upper eyelid. This ‘Lateral Sliding Flap’ technique yielded a good to excellent clinical result in most patients. Although the series needs further extension, in the treated cases it proved – also in the long-term- an efficicaceous and reproducible technique which meets the priorities of eyelid reconstruction, including maximizing the horizontal tension and minimising vertical tension, while replacing the normal eyelid margin at the level of the cornea for optimal visual function and comfort. Compared to the semicircular rotation flap, [2] the lateral eyelid flap results in a shorter vertical scar in the eyelid since a horizontal block excision is performed instead of a pentagonal excision, while respecting the relaxed skin tension lines laterally. In Tenzel’s technique a semicircular rotation skin-muscle flap is used, which results in an unnatural scar that interferes with both the relaxed skin tension lines as well as the draining lymphatics of the upper eyelid. Both techiques share the advantage of creating a continuous proper eyelid margin at the level of the cornea, resulting in an optimal interface for eye comfort and vision. In other techniques, including the (modified) Hughes flap, [6] the sandwich flap by Paridaens & van den Bosch, [1] a technique for reconstruction of upper lid marginal defects by Irvine & McNab [7] or lower lid marginal defects by Moesen & Paridaens, [8] employing vertical advancement of a tarsoconjunctival flap covered with a free skin graft or a skin/muscle acvancement flap, the interface between the lower eyelid margin and the cornea is disturbed, which may cause tear film disturbances resulting in complaints of blurred vision, ocular irritation and redness. This may get worse in case of corneal touch by lanugo hairs arising from the advanced or grafted skin at the level of the lower eyelid margin. In both the lateral sliding flap technique and the semicircular rotation flap technique, longstanding corneal irritation due to interface problems is unlikely. In the early postoperative phase, some irritation may be encountered due to the wound healing at the level of the flap fixation to the remaining eyelid, and one should avoid that any suture material touches the eye during the healing process. From a cosmetic point of view, the presence of lashes in the central eyelid is important. Both the lateral sliding flap and the semicircular flap are techniques in which (at least a subset of) lashes in the central (lower) eyelid are preserved. As the retractors are cut in the lateral sliding flap technique, the resulting short-term vascular insufficiency might explain the occasional loss of (some) eyelid lashes, especially in patients with larger eyelid defects. A reduced horizontal transsection of retractor/conjunctival layer might result in an even better preservation of lashes.
The semicircular flap is used to close small to large pentagonal eyelid defects. The defects that were closed using the ‘Lateral Sliding Flap’ technique were rectangular. There was no need to create a pentagonal defect which has a greater vertical dimension, and –thus- a greater vertical scar following reconstruction.
Various complications of the semicircular flap have been reported, including lateral canthal webbing, ectropion, lid notching, and symblepharon formation [9]. Although we did not encounter complications in our (small) series, we expect these problems may also occur in patients treated with the lateral eyelid flap technique, especially if the flap is inappropriately used in too large defects. Mustardé commented that the sliding flap may drift back, causing a tendency to pulling down of the central scar [3]. In addition, Tyers & Collin mentioned that the tip of the narrow advancement flap may become ischemic or necrotic [4]. The latter was not observed in our study, while contour problems were -at most- acceptable, and did not require additional surgical correction.
Compared to two-staged procedures, the single-stage “Lateral Sliding Flap” and semicircular flap hold the advantage that they are short procedures saving costly operating time. In addition, there is no need for postoperative patching of the patient, which may interfere with daily life activities.
In this study, we showed that the lateral sliding flap may also be used for the closure of upper eyelid defects, as an alternative to the semicircular rotation flap, but more than our two cases are needed before definite conclusions can be drawn. Both the semicircular flap and lateral eyelid flap share the indication spectrum: Lid defects of up to 50% of the horizontal eyelid length. Other one-stage procedures that result in a normal eyelid margin at the level of the cornea, including the “Composite Graft” and “Sandwich Block” techniques [10-13],share the disadvantage of lid-sharing, which results in donor site morbidity and cost more operating time.
Conclusion
we feel that the lateral sliding flap represents a useful technique to close lower and eyelid defects of up to 50% with an optimal postoperative corneal interface and a good cosmetic outcome. Compared to the widely used semicircular flap technique, which has a similar indication spectrum, the lateral sliding flap may have cosmetic advantages due to the “Hidden Incisions”.
Acknowledgements: The author thanks Mrs Jessica Leenen for her artistical input in Fig 1 and Mr Edward Breedveld for his technical support with the figures. Part of this work was presented at the Annual Meeting of the European Society of Ophthalmic Plastic & Reconstructive Surgery (ESOPRS), Stockholm, Sweden, 2017 (Sept 14-16), at the Annual Meeting of the Netherlands Ophthalmology Society (Nederlands Oogheelkundig Gezelschap (N.O.G.)), 2016 (April 6-8), and at the Combined Meeting of the Japanese Society of Ophthalmic Plastic & Reconstructive Surgery (JSOPRS) & the Asia-Pacific Society of Ophthalmic Plastic & Reconstructive Surgery (APSOPRS), Osaka, Japan, 2016 (Aug 26-29).
Funding: This study is supported by a grant from the SWOOFlieringa foundation, Rotterdam.
Ethics approval and consent to participate: The study was approved by the scientific/ethical review board of the Rotterdam Eye Hospital. Consent for publication of patients’ clinical pictures was obtained.
References
- Paridaens D & van den Bosch WA. Orbicularis muscle advancement flap combined with free posterior and anterior lamellar grafts: A 1-stage sandwich technique for eyelid reconstruction. Ophthalmology. 2008; 115: 189.
- Tenzel RR: Reconstruction of the central one half of an eyelid. Arch Ophthalmol. 1975; 93: 125.
- Mustardé JC. Repair and reconstruction in the orbital region: A practical guide. 2nd ed., Churchill Livingstone. 1980.
- Tyers AG and Collin JRO. Colour atlas of ophthalmic plastic surgery. 1st ed. Churchill Livingstone. 1995.
- Verhoekx JSN, Soebhag RK, Weijtens O, van den Bosch WA, Paridaens D (2016): A single- versus double-layered closure technique for full-thickness eyelid defects: A comparative study. Acta Ophthalmol. 94: 257.
- Hughes WL. Reconstruction of the lids. Am J Ophthalmol. 1945; 28: 1203.
- Irvine F & McNab AA. A technique for reconstruction of upper lid marginal defects. Br J Ophthalmol 2003: 87: 279.
- Moesen I & Paridaens D. A tarsoconjunctival advancement flap combined with orbicularis muscle mobilization an a free skin graft: A technique for lower eyelid reconstruction. Br J Ophthalmol. 2007; 91: 1695.
- Miller EA, Boynton JR. Complications of eyelid reconstruction using a semicircular flap. Ophthalmol Surg. 1987; 18: 807.
- Callahan A. The free composite lid graft. Arch Ophthalmol. 1951; 45: 539.
- Hübner H. Kolobomverschluss mittels freier Tarsus-Lidrand überpflanzung. Klin Mbl Augenheilk. 1976; 168: 677.
- Putterman AM. Viable composite grafting in eyelid reconstruction. Am J Ophthalmol. 1978; 85: 237.
- Akdag F, van den Bosch WA, Ganteris E, Paridaens D. Sandwich block for eyelid reconstruction. Orbit. 2010; 29: 110.