
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
The interplay of protective and risk factors linked to autism
Priya Joon1; Anil Kumar*1; Milind Parle2
1Pharmacology Division, University Institute of Pharmaceutical Sciences (UIPS), Panjab University, Chandigarh-110014, India.
2 Pharmacology Division, Dept. Pharm. Sciences, Guru Jambheshwar University of Science and Technology, Hisar (Haryana), Residence: D-2, Pharmacy University (DPSRU), New Delhi, India.
*Corresponding Author : Anil Kumar
Professor of Pharmacology, Pharmacology Division,
University Institute of Pharmaceutical Sciences (UIPS),
Panjab University, Chandigarh-110014, India.
Email: kumaruips@yahoo.com
Received : Mar 15, 2021
Accepted : Apr 23, 2021
Published : Apr 27, 2021
Archived : www.jcimcr.org
Copyright : © Kumar A (2021).
Abstract
Over the last century, Autism has undergone considerable diagnostic evolution. It is only in the past eight years that autism has been identified not as a single disorder but as a “Spectrum” of developmental disabilities inclusive of “Autistic Disorder, Pervasive Developmental Disorder not Otherwise Specified (PDD-NOS), and Asperger’s Disorder”. Autism Spectrum Disorder (ASD) is a complex disorder with early childhood onset, characterized by impairments in reciprocal social interactions and stereotypic behaviors. The limited scientific knowledge about the pathogenesis of ASD has an undesirable impact on the personal, professional, and social life of ASD patients and their families. The interplay of risk factors such as peculiar genetic make-up, adverse environment, etc., and protective factors like proper maternal care and diet appears to be responsible for the development of ASD. Although there is no US-FDA- certified medication for curing autism, an integrated strategy comprising of psychotropic medications and complementary therapies appears to be quite effective. The authors recommend that focusing on the protective factors antepartum and post-partum might prove to be an effective method for the prevention of ASD.
Keywords: Autism; Interplay; Protective; Gynecological; Factors.
Citation: Joon P, Kumar A, Parle M. The interplay of protective and risk factors linked to autism. J Clin Images Med Case Rep. 2021; 2(2): 1070.
Introduction
Autism Spectrum Disorder (ASD) is a lifelong multi-factorial developmental disability manifested by cognitive, behavioral, and social deficits with early childhood onset. ASD is presently considered as one of the most commonly occurring childhood disorders with the global prevalence at 0.62%. The genetic and non-genetic factors play an important role in the etiology of ASD. The diagnosis of ASD has undergone continual developments over the past century and is described explicitly in the fifth version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). The update on the chapter on “Mental, Behavioral and Neurodevelopmental Disorders” in the 11th revision of the “International Classification of Diseases and Related Health Problems” (ICD-11), published by WHO for prospective implementation from January 2022 has aroused immense global curiosity [1]. At present, there is no satisfactory treatment for the core symptoms of ASD viz. defective social interaction and repetitive/stereotypic behavior. Nonetheless, secondary symptoms associated with autism and psychiatric co-morbidities can be diminished to a large extent with the help of drug therapy and non-drug therapy. The presence of a healthy, prosperous, and caring home environment for a lady during pregnancy influences a child’s personality in a conducive manner. This minireview throws light upon the interplay of risk and protective factors in the genesis of ASD.
Risk factors/causes of autism spectrum disorder
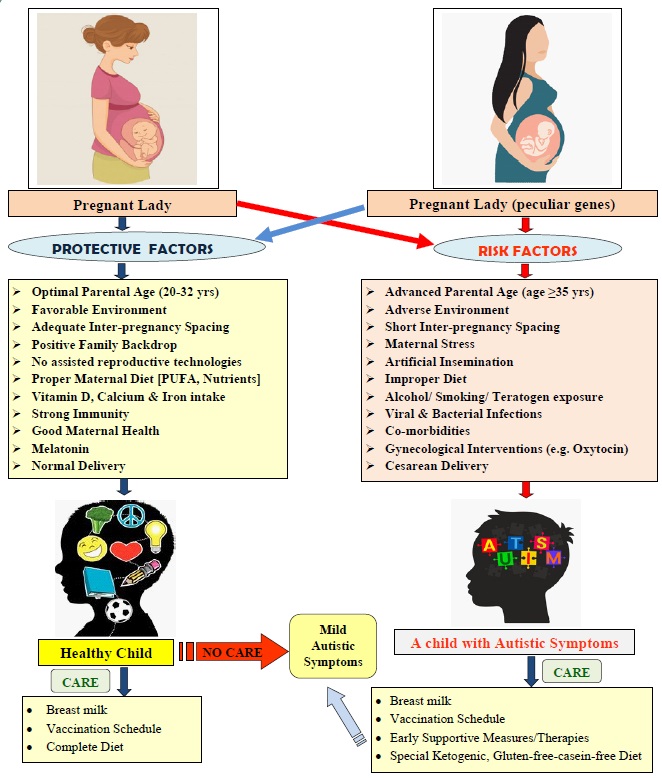
The traditionally acknowledged pathological and non-pathological conditions resulting in ASD include compromised immune system, mitochondrial dysfunction, intellectual disability, prenatal, perinatal, postnatal factors, adverse environment, gynecological interventions, and defective genes, which work independently or in combination to alter the functional capacity of the brain [1,2]. Figure 1 depicts the risk factors and protective factors associated with autism.
Genetics: The actual causative factor of autism is yet not identified. However, genetic make-up appears to play an integral role in causing autism. Several reports suggest that autism could be an inherited disorder. Besides, selected genes play a significant role in the monogenic heritable form of ASD including MeCP2, DbetaH (DBH), and HOXA1. Other genes associated with autistic disorder comprise the FMR-1 gene, Reelin gene, SHANK2, and SHANK3 synaptic scaffolding genes, neuroligins (NLGN3, NLGN4X), neurexin-1 (NRXN1), CNTNAP2 genes, human SLC6A4 gene and human OXTR gene. The genetic architecture of ASD is extremely diverse. Mutated genes interfere with the normal physiological functions including appropriate brain development, synapses, and bones and muscles formation, thereby producing autistic symptoms [3]. No particular gene mutation has been recognized with ASD. However, an individual gene appears to play a very trivial role in ASD, even though more than 400 genes are found to be strongly associated and 200 genes weakly associated. More recent research points to the possibility that ASD is a multi-factorial, multi-pathway genetic disorder that doesn’t obey classical Mendelian inheritance [2]. Advances in computational technologies and data mining are expected to disentangle the genetic aspects of ASD.
Adverse environment: Adverse environment exposure at vulnerable times has attracted the attention of investigators in the area of ASD research. Cumulative neuro-toxicant exposure during sensitive periods of pregnancy may affect neurobehavioral development by disturbing the neuronal circuit formation and causing disorganization of different parts of the fetal brain consequently leading to mental retardation and abnormal behavior in the child. The adverse environment is emerging as a powerful determinant for the development of ASD, although this may be a precipitating factor in individuals having susceptible genes but not a primary causative factor alone (Figure1) [4]. A toxic environment could be an absolute cause of fetal brain damage and may stimulate gene mutation in susceptible individuals. Toxicants suspected to be involved in ASD include insecticides, Polychlorinated Biphenyls (PCBs), harmful wastes, air/ water pollutants, mercury, radiation, diesel exhaust, volatile organic compounds, nitrogen dioxide, and heavy metals [5]. Investigations have been carried out to study the influence of adverse environments at various stages of pregnancy. Interestingly, a link was observed between polluted air and ASD. There was a positive correlation between the cumulative presence of particulate matter in the vicinity of expecting mothers during the third trimester of pregnancy and autism. In another investigation, inter-connection between post-partum nitrogen dioxide (a vehicular-pollutant) and autism was observed [6]. Studies indicate that the pathogenesis of ASD involves a complicated interplay between genetic factors and adverse environment which act synergistically or laterally during vulnerable times of embryonic development, imparting increased sensitivity to the toxic effects of the environment thereby enhancing the probability of developing a child with autism.
Co-morbidities: Co-morbidities often associated with autism, include depression, schizophrenia, schizoaffective disorder, bipolar affective disorder, epilepsy, Down’s syndrome, Tourette syndrome, hypothyroidism, Attention Deficit Hyperactivity Disorder (ADHD), intellectual disorder, metabolic disorders, and hypertension. ASD has been frequently treated as a unique nosological entity, and not as a part of a continuum, which can cover other developmental disabilities. Veritably, the co-occurrence of different disorders seems to be normal rather than the exception. ASD perhaps is not a single disorder, but a blend of common core symptoms accompanied by large variable secondary symptoms characteristic of other co-morbidities [7].
Prenatal, perinatal, and postnatal factors: ASD might be considered, at least in some cases, a disorder of fetal programming.
The prenatal period represents the entire pregnancy duration from conception till delivery of the child. Prenatal development is defined as, “The development of organic structures in a fetus from the moment of conception till birth.” Consumption of medicines (such as thalidomide, valproic acid, misoprostol, acetaminophen) having teratogenic effects, use of alcohol, or tobacco during pregnancy constitutes an important prenatal factor causing ASD [2]. Valproic acid evokes “Fetal Valproate Syndrome” because of enhanced oxidative stress and defective gene expression, which ultimately results in slow development, motor deficits, and abnormal postnatal growth in humans as well as animals [4,8,9]. It is a well-established fact that exposure to certain substances like alcohol, mercury, lead, polychlorinated biphenyls, phthalates, pesticides, insecticides, and radiation during the prenatal period produce autism in children. Maternal infection during pregnancy can result in behavioral abnormalities and neuropathologies in the neonate. There are critical periods during pregnancy when the fetus is immunologically more vulnerable. Furthermore, the teratogenic effects of prenatal infections due to rubella, cytomegalovirus, or Toxoplasma gondii on the central nervous system are well established. Encephalitis due to measles, mumps, herpes simplex virus, varicella, and stealth virus seems to be causally associated with autistic behavior development. Viral or bacterial infection in the first or second trimester of pregnancy enhances the risk of autism in children [10]. Autistic characteristics have also been found to escalate after prenatal exposure to unusually large testosterone concentrations, produced by congenital adrenal hyperplasia. The uterine ambiance has a profound impact on the development of the fetus. The compromised mother’s health can deeply affect the long-term mental and physical health of the developing embryo. Other prenatal factors, like short interpregnancy spacing, abnormal gestational age, multiple pregnancies, gestational hemorrhage, gestational diabetes, and advanced parental age might be linked to an increased incidence of ASD [4,5].
The perinatal period pertains to the period around (immediately before and after) birth. The perinatal period is taken as the period from completion of the 20th week (end of 5th month) of pregnancy to the end of 4 weeks (1st month) after the birth of the child. Perinatal factors of ASD are conjoined with obstetric conditions such as under-weight, abnormal pregnancy duration (pre-term delivery), and birth- asphyxia. Perinatal stress (fetal distress), fetal growth restriction, preeclampsia, umbilical cord complications, chorioamnionitis, acute intrapartum hemorrhage, neonatal encephalopathy, brain trauma, and cesarean delivery are all associated with a high susceptibility to autism [2,4,10].
The postnatal period pertains to the period after the birth of the child till it is two years of age. Postnatal factors include a variety of insults inclusive of auto-immune disorders, jaundice, leaky-gut syndrome, amygdale developmental arrest, oxidative stress, vitamin- D deficiency, heavy metal toxicity, and postnatal infections. These factors are associated with a high incidence of autism [2,10].
Gynecological interventions: Gynecological interventions that are used in the Assisted Reproductive Technologies (ART) such as hormonal stimulation, egg retrieval, in vitro fertilization, intra-cytoplasmic sperm injection, micro-manipulation of gametes, and exposure to the culture medium, could subject the gametes and early embryos to uterine stress and may be associated with an increased risk of developmental disorders [11]. Children conceived using ART are at a higher risk for birth defects including a two-fold increase in epigenetic and imprinted disorders. In reality, artificial insemination, hormonal imbalance, advanced parental age, pre-term deliveries, and low birth weight constitute major risk factors for developing autism. Current research seems to suggest that obstetric interventions, Cesarean Sections (CS), and/or oxytocin-induced labor are all likely to cause ASD in children [4] (Figure 1).
Heavy metal toxicity: Recent ecological studies suggest a critical contribution of metal-toxins in autism. Both Aluminum and Mercury appear to be the main culprits, which can penetrate the blood-brain-barrier and exhibit severe adverse effects on the brain as well as the immune system. Intake of these toxic metals by ladies of child-bearing age enhances the susceptibility of a child to ASD [12]. The continuous presence of mercury as a contaminant in the surrounding environment (air, soil, and water), packed eatables, and seafood increase the likelihood of developing autism symptoms. The toxic effects of mercury poisoning include psychological disturbances, the enhanced occurrence of allergies and apnea, similar to autism symptoms. Elevated heavy metals concentrations (arsenic and mercury) have been detected in the blood and urine of children suffering from autism. Lead, cadmium, aluminum, and arsenic toxicity have also been associated with the development of ASD-like symptoms [13,14].
Dysfunctional immune system: Maternal immune system activation and the production of pro-inflammatory cytokines are risk factors for autism. Pregnancy-induced immune-suppression makes a woman more vulnerable to infections. Mother’s immune responses to prenatal viral exposure involve the formation/release of antibodies. These antibodies elevate maternal interleukin-6 (IL-6) levels which in-turn pass through the fetal’s underdeveloped blood-brain-barrier and interfere with the functioning of genes, thereby causing abnormal behavior after birth. Defective immune responses during sensitive periods of neurodevelopment of the child cause neural dysfunction observed in ASD [15]. Besides, obese and underweight mothers carry an enhanced risk of ASD in the newborn. Maternal obesity results in an activated immune system and inflamed uterine ambiance consequently leading to neurodevelopmental impairments in the offspring. On the other hand, malnutrition of the mother evokes a physiological stress response producing neuronal damage mediated via excessive secretion of proinflammatory factors [16]. Of late enhanced concentrations of maternal cytokines and chemokines during pregnancy have been linked to the development of ASD with intellectual disability in the child [17].
Age of parents: The effects of aging on human genetic traits are well documented, particularly in early embryonic development. There is no clear-cut evidence regarding the advanced age of parents and likelihood of having an abnormal child in the family, although several investigators showed the age of parents’ ≥35 years imparted a higher risk of bearing a child with autism [18]. Furthermore, parents with advanced age had a greater risk of a first-born child being abnormal as compared to the later-born children. The most likely underlying mechanism for older fathers to have an abnormal child can be attributed to lower sperm count due to de novo mutations, precipitated by continuous toxic environmental exposure. Whereas, the multiple reasons for older women to bear abnormal children appear to be hormonal imbalance, incompatible uterus, use of contraceptives, and adverse environment [4]. Advancing age of father adversely interferes with the proper formation of the immune system and the central nervous system. An inter-connection is observed between autism and advanced age of parents, mother’s well-being during pregnancy, and prenatal infection. However, the physical immaturity of parents due to younger age and improper maternal care enhances the incidence of autism. Furthermore, women aged less than 20 years carry a higher risk of giving birth to an abnormal child owing to inadequate intrauterine development of the fetus and preterm delivery [2].
Mitochondrial dysfunction: It is observed that the patients suffering from autism exhibit abnormal functioning of mitochondria although classic features of the mitochondrial disease do not exist. Recent findings suggest mitochondrial dysfunction, impaired energy generation, dysregulated neuro-inflammation, and free radical accumulation as major players in the development of autism. The adverse environment is suspected to be an important risk factor for mitochondrial dysfunction which in turn is responsible for diminished energy levels in patients suffering from ASD. The depletion of reserve mitochondrial energy stores may result in memory deficits and aphasia, frequently observed in autism-diagnosed patients [19].
Protective factors
Protective factors hitherto were thought to be just those attributes such as an impressive Intellectual Quotient (IQ) or outstanding social skills inherited by the individual. Protective factors when identified precisely would play a crucial role in preventing the occurrence of ASD. A healthy environment coupled with proper maternal care and diet during pregnancy helps in the normal growth of neonates and plays an important role in preventing ASD-like symptoms. Pregnant ladies with fatty acid deficiency showed a 40% decrease in ASD risk when their mean daily fatty acid intake was maintained at ≥600 µg in the periconception period and/or during the first month of pregnancy. The increase in Polyunsaturated Fatty Acids (PUFA), especially omega-3 fatty acids, during prenatal maternal diet was associated with a decreased ASD risk. Vitamin D supplements during pregnancy reduced the risk of developing ASD in the offspring [20]. Higher iron and calcium intake during the last phase of pregnancy and particularly during breastfeeding was associated with reduced ASD risk [4,20]. Breast-milk offers the best protection to the child against developing ASD symptoms. Some components of breast milk such as bifidobacteria, lysozyme, lipoxins, glutathione, and anti-inflammatory cytokines are plausibly connected to a decreased risk of ASD [21,22]. Another factor that could play a role as a protective agent is the hormone melatonin. Melatonin synthesis is frequently impaired in children with ASD and their mothers. Therefore, consumption of this hormone during pregnancy could act as a neuroprotective factor, decreasing the risk of neurodevelopmental disorders, including ASD [23]. In addition to the above factors, healthy environment, positive family backdrop, optimal age of parents, adequate inter-pregnancy spacing, limited gynecological interventions, proper maternal care, natural delivery as opposed to cesarean section, and specified vaccination schedules, etc. would go a long way in providing a protective shield against the development of ASD (Figure 1). The authors recommend that focusing on these protective factors during pregnancy might prove to be effective in preventing or diminishing ASD symptoms.
Conclusion
The developments in molecular biology, genetics, and data mining approaches offer new opportunities to unravel the mystery of the pathogenesis of ASD. However, the etiology and pathogenesis of this disorder are still a matter of speculation. The etiology of autism has swung from the "Solely environment" approach of the Bettelheim age to the “Solely Genetic” approach of modern times. ASD is not a single disorder but it encompasses a broad spectrum of disorders resulting from genetic and non-genetic risk factors contributing independently as well as together. Nonetheless, the intricate heterogeneity of ASD appears to be related to the interplay of genetic, environmental, and uterine factors. In recent times, there has been an emphasis on shifting behavioral observations to mechanistic investigations to establish cause-effect relationships. The complexity of ASD can be disentangled by studying the interrelationship of multiple risks and protective factors associated with ASD. The diversity of these factors makes it difficult to determine which factor represents the primary cause and which other factors interact with this primary cause and their possible mechanism of influence. No single therapy/ approach fit exactly in all kinds of patients. An integrated strategy comprising of psychotropic medications and complementary therapies appears to be quite effective given the scenario that there is no US-FDAapproved medicine for the treatment of autism as yet. The authors recommend that focusing on the protective factors antepartum and post-partum might prove to be an effective method for the prevention of ASD.
References
- Joon P, Kumar A, Parle M. What is Autism?. Pharmacological Reports 2021.
- Styles M, Alsharshani D, Samara M, Alsharshani M, Khattab A, et al. Risk factors, diagnosis, prognosis and treatment of autism. Front Biosci. 2020; 25: 1682-1717.
- de la Torre-Ubieta L, Won H, Stein JL, Geschwind DH. Advancing the understanding of autism disease mechanisms through genetics. Nat Med. 2016; 22: 345–361.
- Emberti Gialloreti L, Mazzone L, Benvenuto A, Fasano A, Garcia Alcon A, et al. Risk and protective environmental factors associated with autism spectrum disorder: Evidence-based principles and recommendations. J Clin Med. 2019; 8: 217.
- Hyman SL, Levy SE, Myers SM. Identification, evaluation, and management of children with autism spectrum disorder. Pediatrics. 2020; 145: e20193447.
- Kalkbrenner AE, Windham GC, Zheng C, McConnell R, Lee NL, Schauer JJ, et al. Air toxics in relation to autism diagnosis, phenotype, and severity in a US family-based study. Environ Health Perspect. 2018; 126: 037004.
- Emberti Gialloreti L, Curatolo P. Autism spectrum disorder: Why do we know so little?. Front Neurol. 2018; 9: 670.
- Joon P, Dhingra D, Parle, M. Shatavari: A nature’s gift for autism. Asian J Bio Sci. 2019; 14: 12-21.
- Joon P, Dhingra D, Parle, M. Biochemical evidence for anti-autistic potential of Asparagus racemosus. Int J Plant Sci. 2020; 15: 42-51.
- Wang C, Geng H, Liu W, Zhang G. Prenatal, perinatal, and postnatal factors associated with autism: A meta-analysis. Medicine. 2017; 96: e6696.
- Gao J, He X, Cai Y, Wang L, Fan X. Association between assisted reproductive technology and the risk of autism spectrum disorders in the offspring: a meta-analysis. Sci Rep. 2017; 7: 1-8.
- Schofield K. The metal neurotoxins: An important role in current human neural epidemics?. Int J Environ Res Public Health. 2017; 14: 1511.
- Adams J, Howsmon DP, Kruger U, Geis E, Gehn E, Fimbres V, et al. Significant association of urinary toxic metals and autismrelated symptoms-A nonlinear statistical analysis with cross validation. PloS One. 2017; 12: e0169526.
- Li H, Li H, Li Y, Liu Y, Zhao Z. Blood mercury, arsenic, cadmium, and lead in children with autism spectrum disorder. Biol Trace Elem Res. 2018; 181: 31-37.
- Hughes HK, Mills Ko E, Rose D, Ashwood P. Immune dysfunction and autoimmunity as pathological mechanisms in autism spectrum disorders. Front Cell Neurosci. 2018; 12: 405.
- Andersen CH, Thomsen PH, Nohr EA, Lemcke S. Maternal body mass index before pregnancy as a risk factor for ADHD and autism in children. Eur Child Adolesc Psychiatry. 2018; 27: 139-148.
- Jones KL, Croen LA, Yoshida CK, Heuer L, Hansen R, et al. Autism with intellectual disability is associated with increased levels of maternal cytokines and chemokines during gestation. Mol Psychiatry. 2017; 22: 273-279.
- Wu S, Wu F, Ding Y, Hou J, Bi J, Zhang Z. Advanced parental age and autism risk in children: A systematic review and meta-analysis. Acta Psychiatr Scand. 2017; 135: 29-41.
- Matta SM, Hill-Yardin EL, Crack PJ. The influence of neuroinflammation in Autism Spectrum Disorder. Brain Behav Immun. 2019; 79: 75-90.
- Peretti S, Mariano M, Mazzocchetti C, Mazza M, Pino MC, Verrotti Di Pianella A, et al. Diet: The keystone of autism spectrum disorder?. Nutr Neurosci. 2019; 22: 825-839.
- Bar S, Milanaik R, Adesman A. Long-term neurodevelopmental benefits of breastfeeding. Curr. Opin. Pediatr. 2016; 28: 559-566.
- Tseng PT, Chen YW, Stubbs B, Carvalho AF, Whiteley P, Tang CH, Yang WC, Chen TY, Li DJ, Chu CS, Yang WC. Maternal breastfeeding and autism spectrum disorder in children: A systematic review and meta-analysis. Nutr. Neurosci. 2019; 22: 354-362.
- Jin Y, Choi J, Won J, Hong Y. The relationship between autism spectrum disorder and melatonin during fetal development. Molecules. 2018; 23: 198-206.