
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Laparoscopic intermediate gastrectomy for treatment of non metastatic gastric gastrointestinal stromal tumors located at the posterior wall and lesser curvature
Tommaso Marcucci*; Elena Falsetti; Chiara Genzano; Lorenzo Pandolfini; Romana Laessig; Gian Matteo Paroli; Marco Scatizzi
Department of General Surgery of AUSL Toscana Centro, Santa Maria Annunziata Hospital, Florence, Italy
*Corresponding Author : Tommaso Marcucci
Department of General Surgery of AUSL Toscana
Centro, Santa Maria Annunziata Hospital – Florence,
Italy.
Email: tommaso.marcucci@uslcentro.toscana.it
Received : Mar 15, 2021
Accepted : Apr 23, 2021
Published : Apr 27, 2021
Archived : www.jcimcr.org
Copyright : © Marcucci T (2021).
Citation: Marcucci T, Falsetti E, Genzano C, Pandolfini L, Laessig R, et al. Laparoscopic intermediate gastrectomy for treatment of non metastatic gastric gastrointestinal stromal tumors located at the posterior wall and lesser curvature. J Clin Images Med Case Rep. 2021; 2(2): 1073.
Introduction
Gastrointestinal Stromal Tumors (GISTs) are rare neoplasms but they represent the most common type of mesenchymal tumors found in the Gastrointestinal (GI) tract [1-5]. GISTs arise from the interstitial cells of Cajal, “Pacemaker Cells”, that play a neuromotor role in normal gut motility [3,6]. They account for < 1% of gastrointestinal tumors with an estimated annual incidence of 10 to 20 cases for one million of the general population [1,2]. Treatment has not yet been standardized, but surgical resection remains the mainstay for non-metastatic GISTs [5]. The use of laparoscopic techniques has been widely debated. The biological behavior of these tumors lends itself to laparoscopic resection. The feasibility and safety of mininvasive approaches have been established. Systematic reviews and metaanalysis have showed advantages of laparoscopic approaches compared to open procedures in terms of length of hospital stay, decreased postoperative pain, recovery of intestinal activity and resumption of oral intake. This work reports the results of a Laparoscopic Intermediate Gastrectomy (LIG) with gastrogastric anastomosis packaging performed in three cases of nonmetastatic gastric GIST located at the posterior wall and lesser curvature.
Patients and methods
Between November 2017 and September 2019 three patients with non metastatic submucosal gastric tumors were treated by Laparoscopic Intermediate Gastrectomy (LIG) in our institution (Table 1). Two women and one man of mean age of 56 ± 11.1 years with mean BMI of 26.2 ± 1.8. Prior to surgery, all patients underwent upper endoscopy, followed by Computed Tomography (CT) scan to confirm the diagnosis of gastric submucosal tumor and to exclude adjacent organ involvement that could preclude a laparoscopic approach (Figure 1). The diagnosis was confirmed by Magnetic Resonance Imaging (MRI) in one patient and by Endoscopic Ultrasound with Fine Needle Aspiration (EUS-FNA) in the two other patients. During the surgical procedure in order to reduce the risk of anstomotic leakage in one case (lesser curvature GIST) we used the Indocyanine Green (ICG)-enhanced fluorescence technique to verify the optimal perfusion of both gastric stumps and the anastomotic site. ICG was injected intravenously at a concentration of 0,25 mg/ kg diluted in 10 ml of saline solution after anastomosis creation. Gastric perfusion was assessed using a NIR camera system and considered adequate by the surgical team. The risk stratification of the malignant potential of GISTs is categorized as very low, low, intermediate, or high risks according to National Institutes of Health (NIH) consensus criteria. Mitotic rate is defined according to the number of mitoses per 50 high power fields, the proliferative index was assessed with KI67 and tumor size is defined as the maximum diameter of the resecated tumor. In all three cases the tumor’s localization was facilitated by intraoperative endoscopic procedure.
Table. Patient demographics, clinicopathologic data and surgical outcomes of three patients undergoing LIG
Pt |
Age/Sex |
BMI |
Presentation |
Tumor |
Size |
Operating |
Conversion |
Re-feed (postoperative day) |
Postop. |
Postop. |
Postop. |
NIH |
Recurrences or metastases |
1 46/F 24.2 |
Epigastric |
Posterior wall |
|
123 |
No |
1 |
3 |
|
Very low risk |
None |
|||
2 72/F 28.6 |
Upper |
Posterior wall |
|
152 |
No |
2 |
4 |
5 |
None |
Intermediate risk |
None |
||
|
Epigastric |
Higher lesser curvature |
|
111 |
|
1 |
3 |
3 |
None |
Low risk |
None |
||

Surgical technique (LIG)
Four trocars were placed in all interventions. The procedure starts with the induction of pneumoperitoneum introducing Veress needle at Palmer’s point. An optical bladeless trocar is introduced in abdominal cavity in the supra-umbilical side (10/12 mm). A carbon dioxide insufflation is established through this trocar, with a pressure of 12 mmHg. Three further trocars are positioned under direct vision on the right lumbar side (10/12 mm), left lumbar side (10/12 mm) and right paraxiphoid side (5 mm) (Figure 2). A first exploration of abdominal quadrants allows to exclude peritoneal and liver metastases. The margins of the tumor are identified on the intraluminal side endoscopically-assisted using a gastroscope: on the gastric wall the section lines are traced by the surgeon with bipolar forceps (Figure 3a-c). Greater and lesser gastric curvature vascularisation is transected with ultrasonic device (Harmonic scalpel) and clips (Lapro-Clip), removing the part of omentum of the gastric portion involving the tumor (Figure 3d-f). The posterior gastric wall is completely mobilized dividing all pacreatico-gastric attachements (Figure 3g,h). Proximal and distal section of the stomach is performed using Endo-GIA with Tri-Staple technology (purple charge) (Figure 3i-n). The specimen is extracted through the extension of the umbilical access with endo-bag. A first examination of the specimen confirms section margins macroscopically free from disease. The reconstruction time (Figure 3o-t) is performed using a mechanical stapler device: a side to side gastro-gastric anastomosis on the posterior gastric wall is created using Tristaple 60 mm (purple charge) and the gastrotomy is closed with a continuous double-layer suture (V-Loc 3/0). At the end of the intervention, no abdominal drain is positioned.

Results
The demographics, tumor characteristics and outcomes of the three patients are summarized in the Table. The primary presenting symptoms were upper gastrointestinal bleeding in one case and abdominal epigastric pain in the other two. GIST was at the posterior wall in two patients and at the higher lesser curvature in one patient. All patients underwent Laparoscopic Intermediate Gastrectomy (LIG) and there was no conversion, tumor rupture or significant bleeding during surgery. The intraoperative use of ICG angiography to evaluate gastric perfusion was found to be effective (Figure 4). The mean operating time was 128 ± 17.2 minutes. R0 resection was achieved in all patients. No postoperative complications such as bleeding, leakage, obstruction and intraabdominal abscess occurred. The mean re-feed was 1.3 ± 0.47 days and normal recovery of intestinal activity on average afterwards 3.3 ± 0.47 days. The mean postoperative hospital stay was 3.6 ± 0.94 days. Histopathological examination confirmed GISTs with CD117 and CD34 positivity found in all patients. The mean tumor size was 4.3 ± 1.21 cm. The risk stratification according to NIH consensus criteria were: very low (one case); low (one case); intermediate (one case). All tumors were reported to have a negative resection margin. During a mean follow-up period of 22 ± 9.1 months (range, 10-32 months), there were no recurrences or metastases.

Discussion
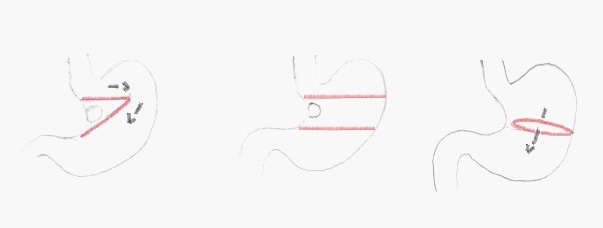
Mazur and Clark first named these mesenchymal tumors as GIST in 1983 and they became more frequently diagnosed around the turn of the century [7]. Firstly classified as leiomyomas, leiomyosarcomas and leyomyoblastomas, thanks to development of immunochemistry and the discover of the tyrosine kinase KIT, GISTs became a separate entity and ther diagnonis increased [8]. GISTs are equally distributed in both sexes. Even if they could be found in patients of all ages, the majority are found in patients between 40 and 70 years old with median age at diagnosis between 60 and 65 years old [2,9,10]. Stomach is the most common site (60%-70%) followed by small bowel (20%-30%) [6,10-13]. Originating from the intestinal pacemaker cell of Cajal, the majority (70%-85%) of GISTs present mutations in the c-KIT proto-oncogene and positivity for CD117 antigen [5]. In gastric GISTs an other commonly expressed marker is CD34 antigen [6,14]. These tumors generally have an expansive growth without submucosal or lymphatic spread. The main route of metastasis is hematogenous, so routine lymphadenectomy is not indicated [1,3,5,6,15-17]. The accepted management of non-metastatic GIST remains surgical resection. The end-point of surgery of GIST is a complete resection without tumor rupture, preservation of an intact capsule to prevent spillage and negative margin to reduce the risk of recurrence and disease progression [1,3,18]. Laparoscopic surgery is becoming a feasibile and safe technique for GIST treatment. This procedure allows lower intraoperative blood loss, reduction of postoperative pain, shorter hospital stay and faster recovery to normal intestinal activity [5,6,19-21]. Lukaszczyk and Preletz described in 1992 the first laparoscopic removal of a gastric GIST found during a cholecystectomy [22]. Since then, others have explored the use of laparoscopy for GIST removal. Currently, laparoscopic resection of gastric GIST is considered a valid alternative to more invasive conventional open surgery thanks to their biological behavior and the development of laparoscopic devices. Several studies compared laparoscopic vs open procedures. The study of Shu et al did not find any difference in terms of operative time and complication rates but underlined that time to bowel function and hospital stay were shorter in laparoscopic procedures [23]. The advantages of laparoscopic surgery vs open procedures are confirmed also in a recent meta-analysis (17 studies including over 700 patients) where in the laparoscopic group there are better results in terms of times to first flatus and shorter hospital stay whitout differences of complication rates and operative times[5]. Koh et al in their meta-analysis of 2013 revealed no differences about margin positivity, local recurrence rates and overall survival [24]. On the other hand a recent thorough review showed better rates in terms of negative margins and recurrences besides complication rates significantly lower in the laparoscopic than open procedures [5]. Regarding resection margins, wide margins were advocated but there has been no correlation with improved survival or recurrence [5,15]. Historically, the optimal margin for adequate resection was thought to be 1-2 cm [1,21,25]. However, recent studies have linked tumor size and mitotic activity, and not extent of resection, as the major factors for recurrence and survival [1,14,15]. The consensus is that a negative macroscopic surgical margins are the most important factor in decreasing the risk of local recurrence and metastatic spread [5]. Obviously, the goal of treatment is a complete resection with negative microscopic margin at the histological examination (R0 resection) [1,15,24]. The indication for laparoscopy based on the GIST size is another hotly debated topic. The consensus statements released in 2004 by the National Comprehensive Cancer Network (NCCN) and The European Society of Medical Oncology (ESMO) limited the use of mini-invasive surgery for GIST less than 2 cm in size in order to avoid tumor rupture and intraperitoneal dissemination [26,27]. Despite these recommendations, several laparoscopic resection are reported in literature for GIST larger than 2 cm with good results without complications. This led to a revision in 2010 of NCCN recommendations extending the indication for laparoscopic resection to GIST up to 5 cm [6]. However there are several studies that describe tumors greater than 5 cm up to 10-20 cm in size laparoscopically resected obtaining similar operative outcomes (preserving capsular integrity) and complication rates as compared to open surgery [1,19,24,28-36]. In our experience we treated medium to large tumors with a mean tumor size of 4.3 ± 1.21 cm. Ultimately, considering the biological behavior of GISTs and the experience gained in many centers, minimally invasive surgery must be considered safe and effective. There are several laparoscopic techniques for resection of these gastric tumors. They ranged from Laparoscopic Wedge Resections (LWR), trans-gastric tumor-everting resection, and formal organ resection depending on the size and location of the tumors with appropriate reconstruction. Laparoscopic Intermediate Gastrectomy (LIG) is indicated for GIST of the gastric body and in particular for those located at the lesser curvature and posterior wall. LWR is an adequate procedure for tumors of the anterior wall but it could be difficult to perform in case of GIST of the posterior wall and in those of the lesser curvature. It needs a good visualization of the tumor and for posterior lesions this could involve a nonradical removal. In this location LIG is easy to perform; the complete resection of the intermediate portion of the stomach allows a sure radicality. As regards the posterior GISTs, another technique is the trans-gastric tumor-everting resection. This procedure requires experience also to obtain a oncological radicality. Furthermore, this technique presupposes the presence of an intraluminal exophytic lesion, an element not necessary for LIG. Especially for posteriorly located lesions, endoscopic guidance can help the surgeon and its use should be emphasized during the operation. In our cases an intraoperative gastroscopy was always performed. Another important aspect to underline is that in case of tumors of the lesser curvature in particular medium or large size (2-5 cm or > 5 cm) and towards the gastro-esophageal junction, use of LIG avoids the risk of gastric stenosis and disorders of stomach motility associated to LWR [37-39] (Figure 5). In fact, LWR in these cases can determine gastric deformity and impairment of motility due to a large removal of the gastric wall [37-39] (Figure 5A). In our opinion LIG with a wide gastro-gastric anastomosis performed with Tristaple 60 mm allows a more effective and physiological transit (Figure 5B). In the patient underwented to LIG for GIST of higher lesser curvature > 3 cm, bowel activity resumed on the fourth postoperative day and after 10 months of follow-up no stenosis or delayed gastric emptying occurred. In addition LIG is a relatively fast technique with a mean operation time of 131 minutes similar to that reported in the literature for LWR (about 125 minutes) [3,40-42]. Formal gastric resection can be a valid procedure for medium/large tumors of the lesser curvature and posterior wall in order to obtain an oncological radicality with negative margins. An intermediate gastrectomy can be also an alternative tecnique to typical gastric resection resulting easier to perform in laparoscopy. LIG lets the physiological transit of food unaltered by means of a gastro-gastric anastomosis without the duodenal switch that can determinate malabsorption syndrome [43]. In our opinion, medium-large GISTs located at the lesser curvature/posterior wall are the main indication to LIG. In our experience LIG is an easily executable, safe and effective procedure. In all cases the histopathological study did not detect a neoplastic proliferation on the resection margins. The risk stratification evaluated on the specimen and according to NIH consensus criteria resulted very low in one case and low and intermediate risk in the other two. None of our patients had any major postoperative complications, such as bleeding, intraabdominal abscess, obstruction and leakage. In literature it has recently been reported that intraoperative indocyanine (ICG) angiography is a feasible technique in the evaluation of intestinal perfusion in laparoscopic surgery and potentially useful in reducing the risk of anastomotic leakage [44,45]. Huh YJ et al in particolar demonstrated the potential role and usefulness of ICG-enhanced fluorescence technique using an NIR camera system as assessment tool for anastomotic vascular perfusion in laparoscopic gastric surgery [46]. In the last LIG performed in 2019, we evaluated the perfusion of the anastomotic site with ICG-enhanced fluorescence technique. This fluorescence assessment method after ICG intravenous injection and using Near-Infrared (NIR) camera imaging, showed a good anastomotic perfusion. At a mean follow-up of 22 ± 9.1 months, all patients were recurrence free. It will be useful in the future with a wider LIG case series to compare this procedure with other laparoscopic techniques such as wedge resection, transgastric resection and formal gastric resection in terms of oncological radicality and post-operative complications.
Conclusions
The surgical management of GIST is based on the principles of maintaining an intact capsule to prevent tumor spillage and obtaining a negative margin to ensure complete excision of localized disease. Thanks to generalized advantages of faster postoperative course, laparoscopic surgery is becoming a feasible and safe tecnique in this patology. Laparoscopic intermediate gastrectomy is indicated for GIST of the gastric body and in particular for those located at the level of the lesser curvature and posterior wall of medium/large-sized. In these cases LIG reduces the risk of stenosis and disorders of stomach motility preserving gastric physiology.
Disclosures: Tommaso Marcucci, Elena Falsetti, Chiara Genzano, Lorenzo Pandolfini, Romana Laessig, Gian Matteo Paroli and Marco Scatizzi have nothing to disclose.
References
- Siow SL, Mahendran HA, Wong CM. Laparoscopic transgastric resection for intraluminal gastric gastrointestinal stromal tumors located at the posterior wall and near the gastroesophageal junction. Asian J Surg. 2017; 40: 407-414.
- Perez EA, Livingstone AS, Franceschi D, Rocha-Lima C, Lee DJ, Hodgson N, et al. Current incidence and outcomes of gastrointestinal mesenchymal tumors including gastrointestinal stromal tumors. J Am Coll Surg. 2006; 202: 623-629.
- Choi SM, Kim MC, Jung GJ, Kim HH, Kwon HC, Choi SR, et al. Laparoscopic Wedge resection for gastric GIST: long-term follow-up results. Eur J Surg Oncol. 2007; 33: 444-447.
- Sircar K, Hewlett BR, Huizinga JD, Chorneyko K, Berezin I, Riddell RH. Interstitial cells of Cajal as precursors of gastrointestinal stromal tumors. Am J Surg Pathol. 1999; 23: 377-389.
- Kim JJ, Lim JY, Nguyen SQ. Laparoscopic resection of gastrointestinal stromal tumors: does laparoscopic surgery provide an adequate oncologic resection?. World J Gastrointest Endosc. 2017; 9: 448-455.
- Demetri GD, von Mehren M, Antonescu CR, DeMatteo RP, Ganjoo KN, Maki RG, et al. NCCN Task Force Report: update on the management of patients with gastrointestinal stromal tumors. J Natl Compr Canc Netw. 2010; 8: S1-41.
- Mazur MT, Clark HB. Gastric stromal tumors. Reappraisal of histogenesis. Am J Surg Pathol. 1983; 7: 507-519.
- Eisenberg BL, Trent JC. Adjuvant and neoadjuvant imatinib therapy: current role in the management of gastrointestinal stromal tumors. Int J Cancer. 2011; 129: 2533-2542.
- Tran T, Davila JA, El-Serag HB. The epidemiology of malignant gastrointestinal stromal tumors: an analysis of 1,458 cases from 1992 to 2000. Am J Gastroenterol. 2005; 100: 162-168.
- Machado-Aranda D, Malamet M, Chang YJ, Jacobs MJ, Ferguson L, Silapaswan S, et al. Prevalence and management of gastrointestinal stromal tumors. Am Surg. 2009; 75: 55-60.
- Miettinen M, Lasota J. Gastrointestinal stromal tumors--definition, clinical, histological, immunohistochemical, and molecular genetic features and differential diagnosis. Virchows Arch. 2001; 438: 1-12.
- Dematteo RP, Gold JS, Saran L, Gönen M, Liau KH, Maki RG, et al. Tumor mitotic rate, size, and location independently predict recurrence after resection of primary gastrointestinal stromal tumor (GIST). Cancer. 2008; 112: 608-615.
- Joensuu H. Gastrointestinal stromal tumors: risk assessment and adjuvant therapy. Hematol Oncol Clin North Am. 2013; 27: 889-904.
- Fletcher CD, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ, et al. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol. 2002; 33: 459-465.
- DeMatteo RP, Lewis JJ, Leung D, Mudan SS, Woodruff JM, Brennan MF. Two hundred gastrointestinal stromal tumors: recurrence patterns and prognostic factors for survival. Ann Surg. 2000; 231: 51-58.
- Joensuu H, Fletcher C, Dimitrijevic S, Silberman S, Roberts P, Demetri G. Management of malignant gastrointestinal stromal tumours. Lancet Oncol. 2002; 3: 655-664.
- Fong Y, Coit DG, Woodruff JM, Brennan MF. Lymph node metastasis from soft tissue sarcoma in adults. Analysis of data from a prospective database of 1772 sarcoma patients. Ann Surg. 1993; 217: 72-77.
- Vetto JT. Role of imatinib in the management of early, operable, and advanced GI stromal tumors (GISTs). Onco Targets Ther. 2009; 2: 151-159.
- Novitsky YW, Kercher KW, Sing RF, Heniford BT. Long-term outcomes of laparoscopic resection of gastric gastrointestinal stromal tumors. Ann Surg. 2006; 243: 738-747.
- Karakousis GC, Singer S, Zheng J, Gonen M, Coit D, DeMatteo RP, et al. Laparoscopic versus open gastric resections for primary gastrointestinal stromal tumors (GISTs): a size-matched comparison. Ann Surg Oncol. 2011; 18: 1599-1605.
- Matthews BD, Walsh RM, Kercher KW, Sing RF, Pratt BL, Answini GA, et al. Laparoscopic vs open resection of gastric stromal tumors. Surg Endosc. 2002; 16: 803-807.
- Lukaszczyk JJ, Preletz RJ Jr. Laparoscopic resection of benign stromal tumor of the stomach. J Laparoendosc Surg. 1992; 2: 331-334.
- Shu ZB, Sun LB, Li JP, Li YC, Ding DY. Laparoscopic versus open resection of gastric gastrointestinal stromal tumors. Chin J Cancer Res. 2013; 25: 175-182.
- Koh YX, Chok AY, Zheng HL, Tan CS, Chow PK, Wong WK, et al. A systematic review and meta-analysis comparing laparoscopic versus open gastric resections for gastrointestinal stromal tumors of the stomach. Ann Surg Oncol. 2013; 20: 3549-3560.
- Cuschieri A. Laparoscopic gastric resection. Surg Clin North Am. 2000; 80: 1269-1284.
- Demetri GD, Benjamin RS, Blanke CD, Choi H, Corless C, DeMatteo RP, et al. NCCN GIST Task Force. NCCN Task Force report: Optimal management of patients with gastrointestinal stromal tumor (GIST)--expansion and update of NCCN clinical practice guidelines. J Natl Compr Canc Netw. 2004; 2: S1-26.
- Blay JY, Bonvalot S, Casali P, Choi H, Debiec-Richter M, Dei Tos AP, et al; GIST consensus meeting panelists. Consensus meeting for the management of gastrointestinal stromal tumors. Report of the GIST Consensus Conference of 20-21 March 2004, under the auspices of ESMO. Ann Oncol. 2005; 16: 566-578.
- Kim KH, Kim MC, Jung GJ, Kim SJ, Jang JS, Kwon HC. Long term survival results for gastric GIST: Is laparscopic surgery for large gastric GIST feasible? World J Surg Oncol. 2012; 10: 230.
- Melstrom LG, Phillips JD, Bentrem DJ, Wayne JD. Laparoscopic versus open resection of gastric gastrointestinal stromal tumors. Am J Clin Oncol. 2012; 35: 451-454.
- Catena F, Di Battista M, Fusaroli P, Ansaloni L, Di Scioscio V, Santini D, et al. Laparoscopic treatment of gastric GIST: report of 21 cases and literature’s review. J Gastrointest Surg. 2008; 12: 561- 568.
- Basu S, Balaji S, Bennet DH, Davies N. Gastrointestinal stromal tumors (GIST) and laparoscopic resection. Surg Endosc. 2007; 21: 1685-1689.
- Novitsky YW, Kercher KW, Sing RF, Heniford BT. Long-term outcomes of laparoscopic resection of gastric gastrointestinal stromal tumors. Ann Surg. 2006; 243: 738-747.
- Tabrizian P, Nguyen SQ, Divino CM. Laparoscopic management and longterm outcomes of gastrointestinal stromal tumors. J Am Coll Surg. 2009; 208: 80-86.
- Sokolich J, Galanopoulos C, Dunn E, Linder JD, Jeyarajah DR. Expanding the indications for laparoscopic gastric resection for gastrointestinal stromal tumors. JSLS. 2009; 13: 165-169.
- Lin J, Huang C, Zheng C, Li P, Xie J, Wang J, et al. Laparoscopic versus open gastric resection for larger than 5 cm primary gastric gastrointestinal stromal tumors (GIST): a size-matched comparison. Surg Endosc. 2014; 28: 2577-2583.
- De Vogelaere K, Van Loo I, Peters O, Hoorens A, Haentjens P, Delvaux G. Laparoscopic resection of gastric gastrointestinal stromal tumors (GIST) is safe and effective, irrespective of tumor size. Surg Endosc.2012; 26: 2339-2345.
- Honda M, Hiki N, Nunobe S, Ohashi M, Kiyokawa T, Sano T, et al. Long-term and surgical outcomes of laparoscopic surgery for gastric gastrointestinal stromal tumors. Surg Endosc. 2014; 28: 2317-2322.
- Xu X, Chen K, Zhou W, Zhang R, Wang J, Wu D, et al. Laparoscopic transgastric resection of gastric submucosal tumors located near the esophagogastric junction. J Gastrointest Surg. 2013; 17: 1570-1575.
- Privette A, McCahill L, Borrazzo E, Single RM, Zubarik R. Laparoscopic approaches to resection of suspected gastric gastrointestinal stromal tumors based on tumor location. Surg Endosc. 2008; 22: 487-494.
- Ishikawa K, Inomata M, Etoh T, Shiromizu A, Shiraishi N, Arita T, et al. Long-term outcome of laparoscopic wedge resection for gastric submucosal tumor compared with open wedge resection. Surg Laparosc Endosc Percutan Tech. 2006; 16: 82-85.
- Lee HH, Hur H, Jung H, Park CH, Jeon HM, Song KY. Laparoscopic wedge resection for gastric submucosal tumors: a size-location matched case-control study. J Am Coll Surg. 2011; 212: 195-199.
- Amin AT, Kono Y, Shiraishi N, Yasuda K, Inomata M, Kitano S. Long-term outcomes of laparoscopic wedge resection for gastrointestinal stromal tumors of the stomach of less than 5 cm in diameter. Surg Laparosc Endosc Percutan Tech. 2011; 21: 260- 263.
- Via MA, Mechanick JI. Nutritional and micronutrient care of bariatric surgery patients: current evidence update.Curr Obes Rep. 2017; 6: 286-296.
- Protyniak B, Dinallo AM, Boyan WP Jr, Dressner RM, Arvanitis ML. Intraoperative indocyanine green fluorescence angiography--an objective evaluation of anastomotic perfusion in colorectal surgery. Am Surg. 2015; 81: 580-584.
- Boni L, David G, Dionigi G, Rausei S, Cassinotti E, Fingerhut A. Indocyanine green-enhanced fluorescence to assess bowel perfusion during laparoscopic colorectal resection. Surg Endosc. 2016; 30: 2736-2742.
- Huh YJ, Lee HJ, Kim TH, Choi YS, Park JH, Son YG, et al. Efficacy of assessing intraoperative bowel perfusion with near-infrared camera in laparoscopic gastric cancer surgery. J Laparoendosc Adv Surg Tech. 2019; 29: 476-483.