
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Skull metastasis originating from adenocarcinoma of the esophagogastric junction
Kimpizi Despina; Triantafyllou Tania*; Theodorou Dimitrios
First Propedeutic Department of Surgery, National and Kapodistrian University of Athens, Hippocration Hospital, 114 Vasilissis Sofias Avenue, 11527 Athens, Greece.
*Corresponding Author : Triantafyllou Tania
First Propedeutic Department of Surgery, National
and Kapodistrian University of Athens, Hippocration
Hospital, 114 Vasilissis Sofias Avenue, 11527 Athens,
Greece.
Email: t_triantafilou@yahoo.com
Received : Mar 15, 2021
Accepted : Apr 23, 2021
Published : Apr 27, 2021
Archived : www.jcimcr.org
Copyright : © Tania T (2021).
Abstract
Esophageal carcinoma usually metastasizes to the liver, distant lymph nodes and lungs. The histological subtype may influence the metastatic sites, with bone metastasis being rather uncommon. This is a report on a patient who presented with adenocarcinoma of the esophagogastric junction and a concurrent skull metastasis.
Keywords: Esophageal cancer; Esophagogastric junction cancer; Skull metastasis.
Citation: Kimpizi D, Triantafyllou T, Theodorou D. Skull metastasis originating from adenocarcinoma of the esophagogastric junction. J Clin Images Med Case Rep. 2021; 2(2): 1074.
Introduction
Esophageal carcinoma is one of the most lethal cancers worldwide. Patients with stage IV esophageal adenocarcinoma have a mean survival of five months. The metastatic sites may vary, but the most frequent tend to be non-regional lymph nodes, the liver and lungs. Bone metastases from esophageal cancer most commonly involve the spine, whereas metastases to the skull are considered extremely rare. In this report, we present a case of a 62-year old male patient, who presented with a skull metastasis at initial diagnosis of adenocarcinoma of the esophagogastric junction (EGJ).
Case description
A 62-year old male presented with symptoms of dysphagia, early satiety and weight loss. He also described a painless mass identified on his forehead with slow growth over the past few months. No neurological symptoms were reported. The clinical examination revealed a firm 2.5 cm nodule on the frontal bone. The rest of the clinical findings were otherwise unremarkable (Figure 1).

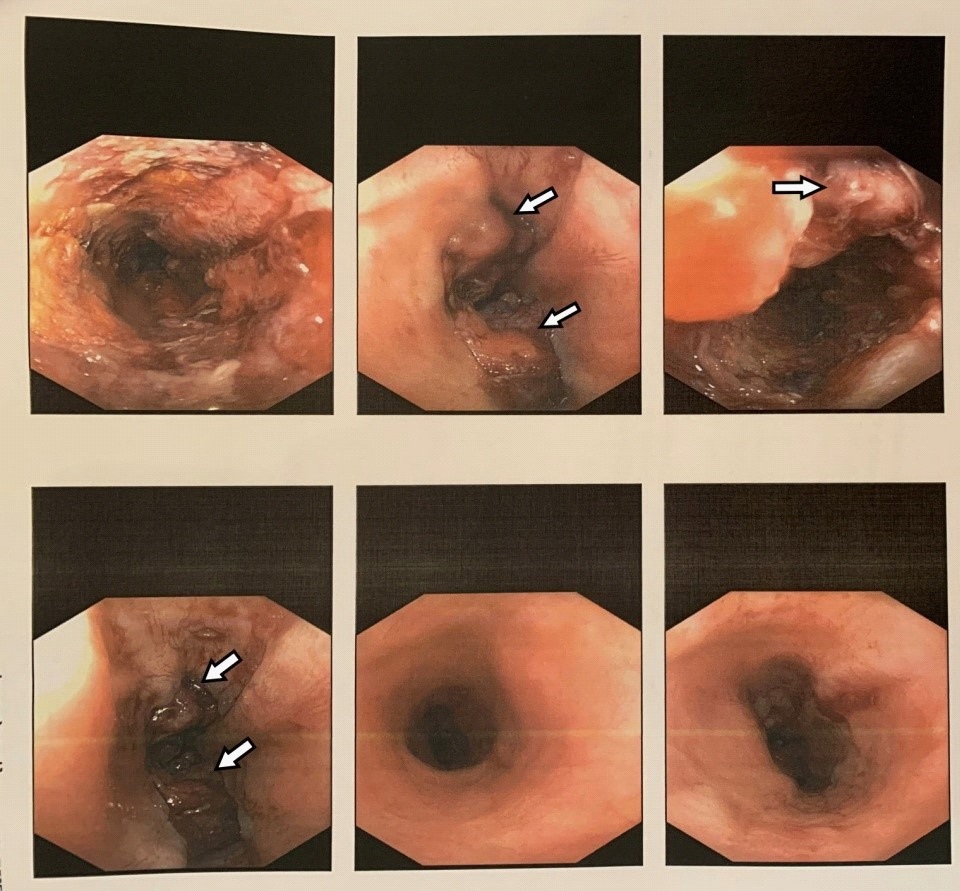
The patient underwent upper gastrointestinal tract endoscopy, which revealed an ulcerated mass extending from 33cm from the upper incisors to the EGJ (Figure 2). Pathologic examination revealed a poorly differentiated intestinal type adenocarcinoma.
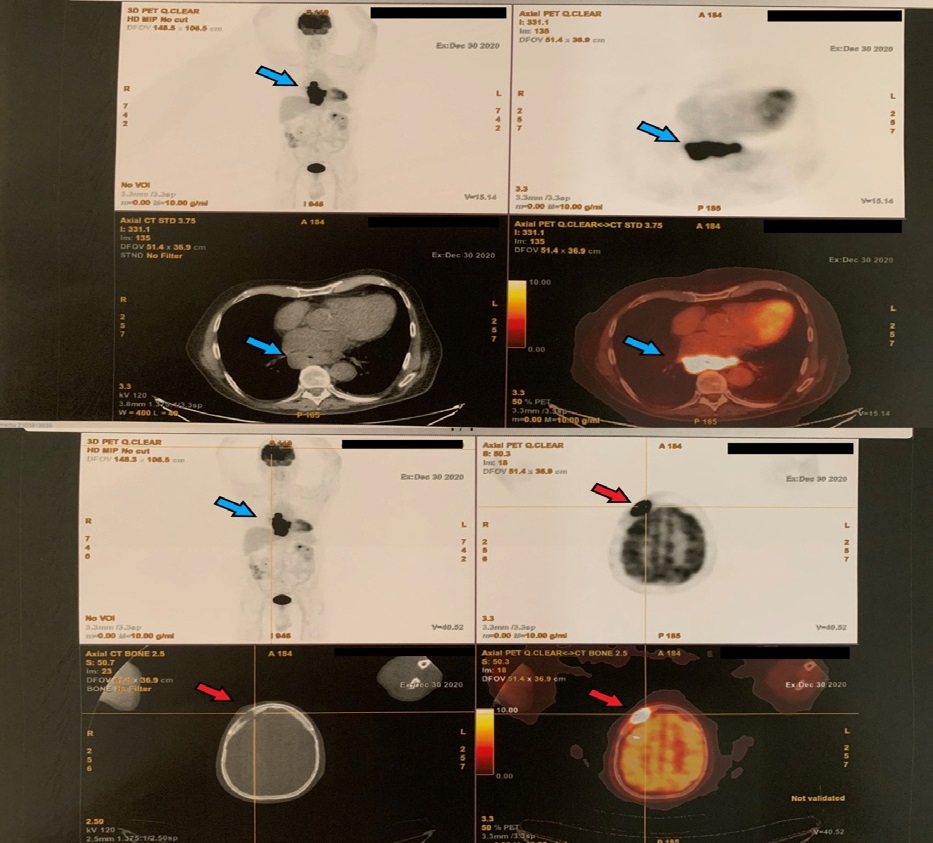
The chest and abdominal Computed Tomography (CT) scans disclosed no metastatic lesions. The patient was further evaluated with 18F-FDG Positron Emission Tomography (PET) scan. Apart from the malignant lesion in the EGJ, the PET scan revealed subcarinal and paraesophageal hypermetabolic lymph nodes. Most importantly, it described a hypermetabolic lytic lesion on the right frontal bone on the anatomic location of the palpable nodule. The SUV max of the 26 X 17 mm mass consisting of soft tissue was 56.7. Bone continuity was disrupted and both superficial and intracranial extension were confirmed. Based on these characteristics and the patient history, the above mentioned lesion was considered metastatic (Figure 3). The patient was referred to the medical oncologist for definite treatment.
Discussion
Patients with stage IV esophageal cancer have poor survival rarely exceeding six months after diagnosis. According to recent population-based studies, the most frequent site of distant metastases from esophageal cancer is the liver, followed by distant lymph nodes and the lung. Skeletal metastases are the fourth most common metastatic site [4,5]. The histological subtype may affect the metastatic pattern and patients’ prognosis. Patients diagnosed with adenocarcinoma more likely present liver metastasis compared to patients with esophageal squamous cell carcinoma. Bone metastases are more frequent in adenocarcinoma, while lung metastases in squamous cell carcinoma [3]. Patients with stage IV adenocarcinoma also tend to have poorer survival when the bone metastases are identified compared to patients with liver metastasis [4].
Skull metastases are extremely rare. Recently, a systematic review studied uncommon metastatic sites of esophageal cancer. The study included 164 patients diagnosed between 1982 and 2017, half of them being staged IV at initial diagnosis. A total of 11 individuals were diagnosed with skull metastases. Our case report describes a rare presentation of metastatic esophageal cancer. Such atypical cases occur occasionally worldwide [1,2]. Furthermore, our report underlines the importance of incorporating a full-body PET scan during staging process aiming to investigate the possibility of distant metastatic sites and individualize the optimal treatment.
References
- Ellis MJ, McDonald PJ. Acute epidural hematoma secondary to skull metastasis from esophageal carcinoma. Can J Neurol Sci. 2007; 34: 491-493.
- Shaheen O, Ghibour A, Alsaid B. Esophageal Cancer Metastases to Unexpected Sites: A Systematic Review. Gastroenterol Res Pract. 2017: 1657310.
- Verstegen MH, Harker M, Van de Water C, Van Dieren J, et al. Metastatic pattern in esophageal and gastric cancer: Influenced by site and histology. World J Gastroenterol. 2020; 26: 6037- 6046.
- Wu SG, Zhang WW, He ZY, Sun JY. et al. Sites of metastasis and overall survival in esophageal cancer: a population-based study. Cancer Manag Res. 2017; 9: 781-788.
- Wu SG, Zhang WW, Sun JY, Li FY, et al. Patterns of Distant Metastasis Between Histological Types in Esophageal Cancer. Front Oncol. 2018; 8: 302.