
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Correlation between surgical findings and magnetic resonance imaging of deep infiltrating endometriosis
Jad Roufael; Benjamin Fedida; Carmen Chis; Anais Guillermin; Penelope Labauge; Pierre Panel
Obstetrics and Gynecology Department, Versailles Hospital Center, 177 rue de Versailles, 78150 Le Chesnay, France.
*Corresponding Author : Jad Roufael
Obstetrics and Gynecology Department, Versailles
Hospital Center, 177 rue de Versailles, 78150 Le
Chesnay, France.
Email: jad.roufael@gmail.com
Received : Mar 16, 2021
Accepted : Apr 23, 2021
Published : Apr 27, 2021
Archived : www.jcimcr.org
Copyright : © Roufael J (2021).
Abstract
In this review, images during surgical excision of Deep Infiltrating Endometriosis (DIE) were correlated to preoperative Magnetic Resonance Imaging (MRI) findings. MRI is known to be the best tool for mapping DIE, it displays a high accuracy in the diagnosis and the characterization of endometriosis lesions. Recent studies showed also that MRI findings can be correlated to the length of operating time, to the duration of hospital stay, and to the risk of voiding problems. In this article we emphasize on the importance of having an experienced radiologist that has the ability of detecting adhesions and superficial peritoneal lesions, a value that was underestimated in previous studies. DIE presents on MRI as an intermediate signal intensity on T1-weighted images, hypointense signal on T2-weighted images, and homo- or heterogeneous enhancement after intravenous gadolinium injection. Preoperative MRI findings help doctors to elaborate a tailored therapeutic plan for each patient depending on the clinical context (Fertility preservation, IVF, complete surgical excisions). Most importantly correct investigation and accurate description of small lesions enhance surgical planification and adequate information of the patients.
Keywords: Deep infiltrating endometriosis; Endometriosis; Laparoscopic findings; Magnetic resonance imaging.
Citation: Roufael J, Fedida B, Chis C, Guillermin A, Labauge P, Panel P. Correlation between surgical findings and magnetic resonance imaging of deep infiltrating endometriosis. J Clin Images Med Case Rep. 2021; 2(2): 1076.
Introduction
Endometriosis is a multifocal gynecologic disease that affects women of reproductive age and may cause chronic pelvic pain and infertility. Deep infiltrating endometriosis is defined as a sub-peritoneal lesion more than 5mm deep. It can affect the parametrium, uterosacral ligaments, rectovaginal septum, rectum, vagina or the bladder [1,2]. Menstrual reflux has a major role in the pathophysiology of endometriosis, and this explains the predominance of the lesions in the posterior compartment of the pelvis and its asymmetric distribution.
Other physio-pathological theories have been proposed such as the theory of vascular and lymphatic emboli and the theory of Mullerian metaplasia [3,4]. Recent studies suggest that DIE represents a unique entity of extrauterine endometriosis with enhanced pro-proliferative and angiogenetic characteristics [5]. It can be responsible of a variety of symptoms like dysmenorrhea, chronic or cyclic pelvic pain, dyspareunia, dysuria and dyschezia. One of its major complication is infertility. Treatment options include In-Vitro Fertilization (IVF), surgery, or a combination of both. The treatment of choice in case of endometriosis associated with infertility is currently investigated in multiple trials. MRI is definitely an important tool for the diagnosis of endometriosis, but all begins with a careful clinical exam and a transvaginal ultrasound which is the first imaging modality. The final diagnosis is obtained after surgery by histopathology of the lesion. In this article we will show you the correlation between MRI and per operative findings [6,7,8]. It is to be noted that all images were analyzed prospectively by a specialized radiologist.
Magnetic resonance imaging protocol
All patients known or suspected to have endometriosis undergo pelvic MR imaging after injection of water in the rectum and sterile gel in the vagina. This technique allows a better visualization of the entire rectal and vaginal interface with the uterus (to be noted that no injection was done for this patient to respect patient’s preferences). Patients undergo the following protocol: Axial, sagittal and coronal high resolution T2-weighted sequences. Axial and sagittal T1-weighted sequences with and without fat suppression.
DIE can affect the uterosacral ligaments, rectovaginal septum, the vagina, urinary tract, alimentary tract, diaphragm and other extraperitoneal sites. Accurate preoperative localisation of the disease is required for planning complete surgical excision. The major two signs of deep infiltrating endometriosis on magnetic resonance imaging are signal intensity abnormalities and morphologic changes. Fibrosis and adhesions often result in morphologic changes, such as, nodular thickening of uterosacral ligaments, intermediate or high signal intensity of DIE lesions on T1-weighted images and hypointense lesions on T2-weighted images. Mild to moderate enhancement may be observed after gadolinium injection. The high sensitivity and specificity of MR Imaging was already discussed in the literature [9,10]. In addition, MR imaging can guide treatment decisions by showing the extension of the disease and all the organs that are involved in the abdomen (ureters, appendix, diaphragm).
Case presentation
A 33-year-old patient, with no medical or surgical history presents to our clinic for primary infertility, dysmenorrhea, dysuria, pollakiuria and deep positional dyspareunia. Patient was asymptomatic when she was on OCPs, however OCPs were stopped two years ago for the interest in becoming pregnant. Basic workup for organic causes of infertility was negative for her and her partner. However, given her symptoms, endometriosis was suspected, and clinical examination was pertinent for left and right uterosacral ligament retraction.
Magnetic resonance imaging showed
Figure 1: Left uterosacral and left round ligament infiltration (nodular thickening) on sagittal T2-weighted images (A). Right and left uterosacral ligaments thickening on transverse T2- weighted images (B,C).
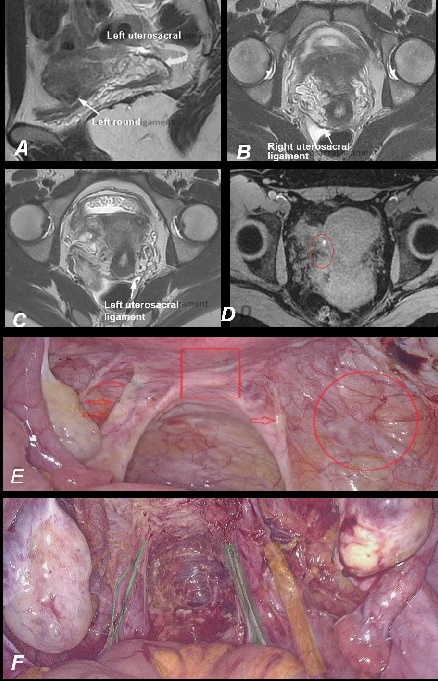
Figure 2: Right and left nodular hyper intensity representing endometriosis implants in the right and left ovarian fossa on transverse T1-weighted images (A,B). We identified also a 7mm right ovarian endometrioma (nodular hyper intensity on transverse T1-weighted images (nodular hyper intensity inside the limits of the ovary) (B).
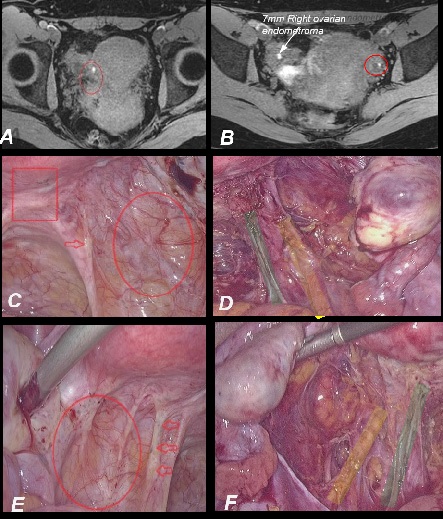
Figure 3: Superficial endometriosis lesions of the “Douglas Pouch” on transverse T2-weighted image.
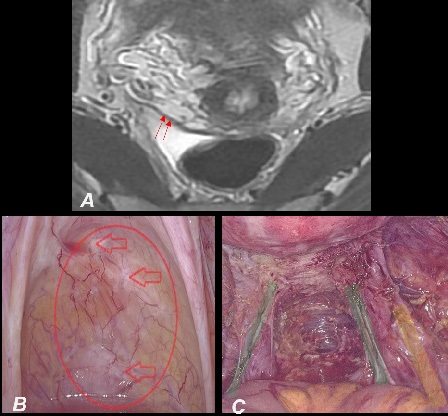
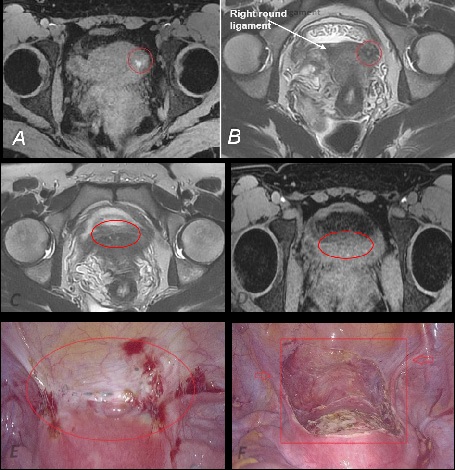
Figure 4: Endometriosis infiltration of the left round ligament represented by a nodular hyper intense lesion on transverse T1 weighted image (A), nodular hypo intense lesion on transverse T2-weighted image (B). Infiltration and thickening of the right round ligament on transverse T2-weighted image (B). Endometriosis infiltration of the uterovesical fold with retraction, fibrosis and hemorrhagic peritoneal spots on transverse T1 and T2- weighted images (C,D).
All endometriosis lesions seen on MRI were identified during surgery. We performed a complete laparoscopic resection of all endometriosis lesions; no complication was noted during or after the surgery. Patient was evaluated two months after surgery; she noted the complete resolution of her symptoms, no dyspareunia, pollakiuria or dysuria.
Surgical procedure
The installation features included a uterine manipulator, a 12 mm trans- umbilical trocar for camera, two 5 mm trocars (in right and left iliac fossa) and another one in the hypogastric region. Multiple endometriosis lesions were identified after a careful examination of the peritoneal cavity.
Posteriorly, endometriosis was found to be infiltrating
- Douglas pouch: white “Stellar” lesions and peritoneal retraction (Figure 3: A).
- Torus: reddish, “powder-burn” lesions and peritoneal retraction (Figure 1: E).
- Right and left ovarian fossa: red and white “Stellar” lesions, peritoneal retraction and increased vascularisation
(Figure 2: C,E).
- Uterosacral ligaments: dark black lesions, fibrosis and retraction causing deep positional dyspareunia (Figure 2: C,
E).
At the level of the anterior compartment, we found endometriosis infiltration of:
Left and right round ligaments: large hemorrhagic lesions
predominating on the right side, yellowish spots, retraction and fibrosis (Figure 4: E).
Uterovesical fold: Yellowish, dark and smaller red spots,
plus retraction and fibrosis of the peritoneal fold (Figure
4: E).
To be noted that all these lesions were identified on MR imaging preoperatively as we showed before. After mobilization of the sigmoid and identification of the landmarks on the pelvic wall, which are the nerves, ureter, and pelvic vessels, we did a bilateral ureterolysis and resection of the right and left ovarian fossa (Figure 2: D,F). Then a bilateral uterosacral ligament resection was done sparing the hypogastric nerves on both sides (Figure 1: F). A complete resection of the Douglas pouch was achieved after opening the para rectal spaces, medially from the uterosacral ligaments, in order to avoid injury to the hypogastric nerves (Figure 3: C). After that, we opened the vesico-vaginal space and we performed a complete resection of the utero-vesical peritoneal fold (Figure 4: F). To be noted that the use of uterine manipulator helps identifying different pelvic structures and decreases surgical complications.
Discussion
Endometriosis may be difficult to identify on MR imaging especially for mild and superficial lesions. As we can see in “Figure 1, 3” the infiltration of the “Douglas pouch and the uterosacral ligaments” is subtle especially in the absence of clear morphologic changes. In our department of Obstetrics and gynecology we systematically conduct multidisciplinary meetings to correlate preoperative and postoperative findings. This allows clinical discussion of the medical case and helps gynecologists and radiologists in improving their skills to offer the best patient care. In this case all endometrial lesions found during surgery were already described and mapped by our experienced radiologist. MR imaging is useful in guiding and planning surgical treatment for the disease. Having an exact mapping of the lesions allows surgeons to be better prepared for the surgical act especially when multiple surgical specialties are involved (ex: colostomy, ureteral stenting). It allows also patients to be better informed regarding their length of hospital stay, clinical outcome. etc.
Conclusion
Correlation between surgical findings and magnetic resonance imaging of deep infiltrating endometriosis may have a positive impact on the treatment of patients suffering from endometriosis. In this article we want to focus also on the importance of referring patients to surgeons who are frequently dealing with endometriosis like in our referral centre at “Versailles Hospital Centre” as this will increase the chances of having a complete endometriosis resection and a better clinical outcome. Most importantly correct investigation and accurate description of small lesions enhance surgical planification and adequate information of the patients.
References
- Koninckx PR, Ph D, Suggestive evidence that pelvic endometriosis is a progressive disease, whereas deeply infiltrating endometriosis is associated with pelvic pain. Fertil. Steril. 1991; 55: 759- 765.
- Luciano DE, Luciano AA. Management of endometriosis-related pain: An update. 2011; 7: 585-590.
- Borghese B, Santulli P, Marcellin L, Chapron C. Definition, description, clinicopathological features, pathogenesis and natural history of endometriosis: CNGOF-HAS Endometriosis Guidelines. Gynecol. Obstet. Fertil. Senol. 2018; 46: 156–167.
- Viganò P, et al. Cellular Components Contributing to Fibrosis in Endometriosis: A Literature Review. J. Minim. Invasive Gynecol. 2020; 27: 287–295.
- Perricos A, et al. Does the Use of the ‘Proseek® Multiplex Oncology I Panel’ on Peritoneal Fluid Allow a Better Insight in the Pathophysiology of Endometriosis, and in Particular Deep-Infiltrating Endometriosis?. J. Clin. Med. 2020; 9: 2009.
- Tang X, et al. Deep infiltrating endometriosis MR imaging with surgical correlation. 2018; 8: 187–195.
- Frate GD, Bazzocchi M, Zuiani C. Pelvic Endometriosis: MR Imaging Appear- ance with Laparoscopic. 2006; 1705–1719.
- Ludovico Muzii PBP, Tucci CD, Galati G, Mattei G, Chiné A, et al. Endometriosis- associated infertility: Surgery or IVF?. Minerva Ginecol. 2021.
- Bazot M, et al. Deep pelvic endometriosis: MR imaging for diagnosis and prediction of extension of disease. Radiology. 2004; 232: 379-389.
- Hottat N, et al. Endometriosis: Contribution of 3.0-T pelvic MR imaging in preoperative assessment-initial results. Radiology. 2009; 253: 126–134.