
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Familial aggregation of COVID-19 severity suggests a genetic component to host infection response
Alexandre R Vieira
Department of Oral Biology, University of Pittsburgh School of Dental Medicine, Pittsburgh, PA 15261, USA.
*Corresponding Author : Alexandre R Vieira
Department of Oral Biology, University of Pittsburgh
School of Dental Medicine, Pittsburgh, PA 15261, USA.
Email: arv11@pitt.edu
Received : Mar 18, 2021
Accepted : Apr 23, 2021
Published : Apr 27, 2021
Archived : www.jcimcr.org
Copyright : © Vieira AR (2021).
Abstract
Familial aggregation of COVID-19 cases suggest transmission occurs by contact but can also be evidence of a genetic component to the disease presentation. The goal of this work was to evaluate the disease pattern in families that many individuals have been affected by the disease. A case series analysis of six families that had many individuals affected by COVID-19 and the pattern of the severity of the disease is reported. Families were from two densely populated cities in Brazil. Participants included family members of six unrelated families, with some individuals that showed signs of COVID-19. The exposure was SARS-CoV-2 in the same household. The main outcomes and measures were disease affection and severity, including mortality. From the six families, two had mild cases only, whereas the other four families showed severe disease and death in the same sibship. The two families that had mild disease could be followed for six months and one showed reinfection after six months. This cases series suggest that disease severity aggregates in families, which suggests a genetic component for individual host response to SARS-CoV-2 infection.
Keywords: Sars-Cov-2; Familial Aggregation; Corona virus.
Citation: Vieira AR. Familial aggregation of covid-19 severity suggests a genetic component to host infection response. J Clin Images Med Case Rep. 2021; 2(2): 1077.
Introduction
COVID-19 has quickly become a worldwide issue, primarily due to its contagious nature. Transmission from family members in the household [1-9] is likely one of the biggest challenges for proposed measures of physical distancing and lockdowns that many countries have adopted, particularly for the segments of populations that are less economically favored. The term familial aggregation has been used to indicate the transmission of SARS-CoV-2 within families living in the same household. Familial aggregation has also an implicit meaning of an underlying contribution of genetic factors, and has been widely used in the literature in such manner in the case of other conditions.
Evaluation of genetic variants that may modulate how infection by SARS-CoV-2 impacts the host has suggested that an epithelial-specific transcriptional repressor implicated in airway disease (EHF) is associated with SARS-CoV-2 infection [10]. Patients with blood group A were reported to have an increased risk for infection with SARS-CoV-2, whereas blood group O was associated with a decreased risk, indicating that certain ABO blood groups may be correlated with SARS-CoV-2 susceptibility [11]. Furthermore, a gene cluster in 3p21.31 was associated with COVID-19 with respiratory failure, and a potential involvement of the ABO blood-group system in 9q34.2 was again suggested when association tests throughout the genome were implemented [12]. The elucidation of a genetic component will likely provide additional insight on how the disease can be managed, and in this report, we provide evidence that COVID-19 clinical severity aggregate in families.
Case series
Ethics
Written informed consent was obtained from the individual(s) AND/OR minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this report.
Families
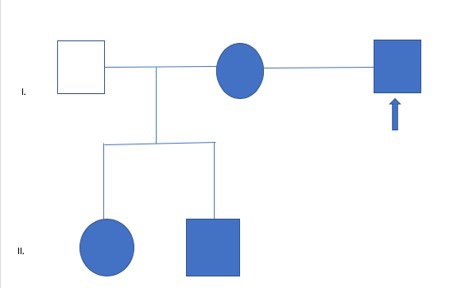
Family 1 (Figure 1) lives in the city of Rio de Janeiro and is predominantly of Jewish/European descent. Individual I-3 (58 years old), who was in the same household, without the possibility of complete isolation, as I-2 (45 years old), II-1 (21 years old), and II-2 (17 years old), was the source of the infection to the others. Individuals II-1 and II-2 went to be under the care of I-1 (50 years old) in a different household, who was certainly exposed to SARS-CoV-2 but did not contract COVID-19. All affected had relatively mild symptoms with fever, fatigue, cough, and shortness of breath. Individual II-1 had mild to moderate symptoms but did not seek hospital care.
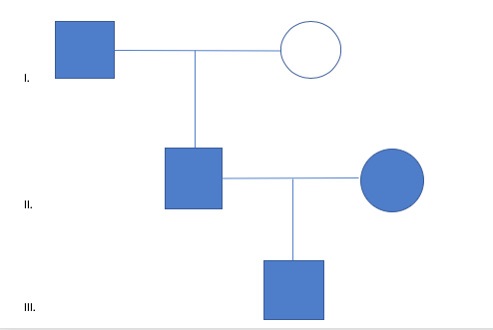
Family 2 (Figure 2) lives in the city of Rio de Janeiro and is of Portuguese descent. It is unclear which individual was the source of the infection and all live in the same household without the possibility of complete isolation. I-1 (81 years old), II-1 (49 years old), II-2 (40 years old), and III-1 (14 years old) all showed mild signs of COVID-19 (cough and fatigue). Individual I-2 (79 years old) was certainly exposed but did not show any signs of the disease.
Family 3 lives in the metropolitan area of Rio de Janeiro and includes a mother of four that was admitted to the emergency room with a heart attack, and died soon after. She is of AfricanEuropean mixed descent and two days later, her older son (45 years of age) and her younger son (35 years of age) were admitted to the same hospital with symptoms of COVID-19 and died soon after in the same day.
Family 4 lives in the metropolitan area of Rio de Janeiro and is mixed of African and European descend. After attending a family gathering, seven individuals of the family without reported concomitant diseases (the oldest, a female 91 years of age, and the youngest, a male 39 years of age) showed signs of COVID-19 and developed severe respiratory symptoms. All seven died in the span of two weeks.
Family 5 lives in the metropolitan area of Rio de Janeiro and is of Portuguese descent. Three siblings died in two days, a 71-year-old female that tested positive for COVID-19 and died of heart failure, the middle brother that died of complications of COVID-19, and the younger sister, who died of complications of diabetes and no signs of COVID-19. The 45-year-old son of the older sister, who was wheel chair bound and also had diabetes, also died from complications of COVID-19.
Family 6 lives in the metropolitan area of São Paulo and is mixed of African and European descend. Twenty-eight members attended a birthday party of a woman relative, which included her six siblings. Soon after, 14 family members showed signs of COVID-19. The woman celebrating her 59th birthday and her husband (61 years of age) showed signs of COVID-19 and died soon after the party. Further, two of her male siblings, an older one (62 years of age) and a younger one also died of COVID-19. There were no reports of concomitant diseases affecting the four individuals who died. The remaining ten COVID-19- affected family members recovered.
6-Month follow-up of families 1 and 2
It was possible to follow families 1 and 2 (Figures 1 and 2) after they recovered from their initial infection. Family 2 continued COVID-19 free after 6 months, whereas individuals I.2, I.3, and II.2 showed signs of COVID-19 reinfection. I.2 and I.3 had mild symptoms whereas II. 2 reported symptoms that were more severe than the first time he was infected. Individuals I.1 was once again exposed to his son but did not show any signs of contracting the disease.
Discussion
The evaluation of these six families suggest that mild disease, as well as severe COVID-19 that leads to death aggregate in families, indicating a genetic component. This evidence allows us to speculate that possibly genetic mechanisms that inhibit the virus to efficiently infect cells of the host or an efficient immune response that some hosts show when infected by COVID-19 exist. In some instances, as can be seen in families 1 and 2, some individuals may be even “Protected” against SARS-CoV-2 infection. Similarly, people may be more susceptible to a more severe disease trajectory, that increases the odds of death, and that as well aggregates in families, as can be seen for families 3, 4, 5, and 6. Family 5 shows that diabetes was a concomitant condition in some individuals and the severity of COVID-19 outcome may be related to an increased ACE2 expression, which may influence susceptibility to more severe infection [13].
Conclusions
These series of six families provide evidence that the host response to SARS-CoV-2 infection is similar within nuclear families, suggesting a genetic component.
References
- Bai SL, Wang JY, Zhou YQ, Yu DS, Gao XM, et al. Analysis of the first cluster of cases in a family of COVID-19 in Gansu province. Zhonghua Yu Fang Yi Xue Za Zhi. 2020; 54: 491-493.
- Chen J, Wang X-F, Zhang P-F. Asymptomatic SARS-CoV-2 infection in children: A clinical analysis of 20 cases. Zhongguo Dang Dai Er Ke Za Zhi. 2020; 22: 414-418.
- Tan X, Huang J, Zhao F, Zhou Y, Li J-Q, et al. Clinical features of children with SARS-CoV-2 infection: An analysis of 13 cases from Changsha, China. Zhongguo Dang Dai Er Ke Za Zhi. 2020; 22: 294-298.
- Wu H-P, Li B-F, Chen X, Hu H-Z, Jiang S-A, et al. Clinical features of coronavirus disease 2019 in children aged <18 years in Jiangxi, China: An analysis of 23 cases. Zhongguo Dang Dai Er Ke Za Zhi. 2020; 22: 419-424.
- Xia X-Y, Wu J, Liu H-L, Xia H, Jia B, Huang W-X. Epidemiological and initial clinical characteristics of patients with family aggregation of COVID-19. J Clin Virol 2020, 127, 104360.
- Yao Y, Tian Y, Zhou J, Ma X, Yang M, et al. Epidemiological characteristics of SARS-CoV-2 infections in Shaanxi, China by 8 February 2020. Eur Respir J. 2020; 55: 2000310.
- Zhang H-Y, Zhang Y. Coronavirus disease 2019 and hypertension in 2 children. Zhongguo Dang Dai Er Ke Za Zhi. 2020; 22: 425- 428.
- Zhang SX, Li J, Zhou P, Na JR, Liu BF, et al. The analysis of clinical characteristics of 34 novel coronavirus pneumonia cases in Ningxiu Hui autonomous region. Zhonghua Jie He He Hu Xi Za Zhi. 2020; 43: 431-436.
- Zheng F, Tang W, Li H, Huang Y-X, Xie Y-L, Zhou Z-G. Clinical characteristics of 161 cases of corona virus disease 2019 (COVID-19) in Changsha. Eur Rev Med Pharmacol Sci. 2020; 24: 3404-3410.
- Kachuri L, Francis SS, Morrison M, Bossé Y, Cavazos TB, et al. The landscape of host genetic factors involved in infection to common viruses and SARS-CoV-2. medRxiv. 2020; 05.01.20088054.
- Wu Y, Feng Z, Li P, Yu Q. Relationship between ABO blood group distribution and clinical characteristics in patients with COVID-19. Clin Chim Acta 2020. S0009-8981(20)30290-4.
- Ellinghaus D, Degenhardt F, Bujanda L, Buti M, Albillos A, et al. for The Severe Covid-19 GWS Group. Genomewide association study of severe covid-19 with respiratory failure. New Engl J Med. 2020: 383; 1522-1534.
- Rao S, Lau A, So H-C. Exploring diseases/traits and blood proteins causally related to expression of ACE2, the putative receptor of SARS-CoV-2: A Mendelian randomization analysis highlights tentative relevance of diabetes-related traits. Diabetes Care. 2020; 43: 1416-1426.