
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Nuclear odontology: Pictorial essay
Saleh A Othman
Nuclear Medicine Division, Department of Radiology and Medical Imaging, King Khalid University Hospital and College Of Medicine, King Saud University, 7805(46), Riyadh 11472 - Saudi Arabia.
*Corresponding Author : Saleh A Othman
Nuclear Medicine Division, Department of Radiology
and Medical Imaging, King Khalid University Hospital and College Of Medicine, King Saud University,
7805(46), Riyadh 11472 - Saudi Arabia.
Email: sothman@ksu.edu.sa
Received : Mar 11, 2021
Accepted : Apr 26, 2021
Published : Apr 29, 2021
Archived : www.jcimcr.org
Copyright : © Othman S (2021).
Abstract
There is increased demand by the general dentist and oral surgeon’s for Nuclear Medicine (NM) imaging procedures both for initial diagnosis and follows up of patients with different dental and facial disorders. There are several procedures in NM including bone scan, gallium scan and PET scan which can offer important diagnostic information complementing the information obtained from other imaging modalities in particular a better understanding of the pathophysiology of the disease and therapy monitoring.
Citation: Othman SA. Nuclear odontology: Pictorial essay. J Clin Images Med Case Rep. 2021; 2(2): 1080.
Introduction
During the last two decades, I have witnessed increased demand by the general dentist and oral surgeon’s for Nuclear Medicine (NM) imaging procedures both for initial diagnosis and follow ups of patients with different dental and facial disorders. This fact inspired me to call this work ‘Nuclear Odontology’ terminology to the best of my knowledge not stated before.
Nuclear odontology is the use of Nuclear Medicine (NM) in the diagnosis of dental and oral disorders. NM is a branch of medicine in which small quantities of radioactive material is given to the patient mainly through an intravenous route to assess the function of organs rather than the structure which is best evaluated by anatomic imaging such as Computed Tomography (CT) and Magnetic Resonance Imaging (MRI). Therefore if we want to assess the size and location of temporal condyle we perform a CT scan, however to assess the osteoblastic activity of the condyle bone scan gives the answer. The aim of this essay is to familiarize the general dentist and oral surgeon who are not acquainted and refresh those who are with the available NM imaging procedure which can help them in their daily practice. In addition we will discuss the application of NM in several disorders of the dental and oral cavity which the physician may face in daily practice of odontology.
Methods
There are several procedures in NM used for the diagnosis and follow up of dental and oral disorders including bone scan, gallium scan and PET scan.
Imaging techniques
The images obtained can be planar images (two dimension) or tomographic images (three dimension): Single Photon Emission Computed Tomography (SPECT) coupled with Computed Tomography (CT) and fused together to give SPECT/CT image. The other modality is Positron Emission Tomography (PET) and when fused to CT gives PET/CT image. The studies presented in this review were done in our department. Planar and SPECT/ CT was performed using a dual head gamma camera (Philips’ Bright View XCT). PET /CT performed using (General Electric Discovery ST 64-slice PET/CT machine system).
The radioactive materials used for diagnostic purposes are of short half-life and therefore there is no significant hazard to the patients or to the staff managing them.
Imaging protocols
Bone scan: Three phases bone scan (blood flow, blood pool and uptake phase) is performed when infection suspected and images obtained immediately post injection for blood flow and blood pool images and a delayed planar scan is obtained 2-3 hours post intravenous injection of 20-25 millicurie (mCi) 99mTC-methylene diphosphonate (99 mTC-MDP) which accumulates on the surface of the bone mineral matrix. The bone uptake of the tracer depends on blood flow and metabolic bone activity. No patient preparation is required. The patient is instructed to drink plenty of fluid and empty the urinary bladder frequently to reduce radiation dose. SPECT/CT is performed to the area of interest.
Gallium-67 scan: Gallium-67citrate (Ga-67) binds to transferring, lactoferrin, leukocytes and siderrophores produced by bacteria and accumulates in infection and inflammatory sites. The patient is injected intravenously 4.0-5.0 mCi Ga-67 and planar images obtained 48 hours postinjection coupled with SPECT/CT image to the area of interest.
PET/CT: F-18 FDG: Fluoro Deoxy Glucose (FDG) labeled with Fluorine -18 (F-18) is the most widely used PET radiopharmaceutical for tumor imaging. F-18 FDG is taken up by cells in proportion to their metabolic rate. In tumors there is increased glycolysis compared to normal cells leading to high target (tumor) non target (normal cells) ratio.
The patient in fasting state, PET/CT images are obtained 60 minutes post intravenous injection of 10 mCi F-18 FDG.
Clinical applications
Plain radiograph, panorama imaging, cone beam CT, CT and MRI are the most commonly used techniques by dentists and oral surgeons. However, these are anatomic imaging techniques which reveal changes in structure and they have some limitations in post-operative conditions where differentiation between residual or recurrent disease from scarring is a challenge. Nuclear medicine and after the recent introduction of hybrid imaging (SPECT/CT, PET/CT and PET /MR) has the power to solve this dilemma hence it evaluate changes in function (which precedes changes in structure) and structure as well to determine disease extent and in neoplastic lesions assess local extension and distant metastases at initial stage of the disease (staging), monitoring therapy (therapy response) and follow up and detection of recurrence(re-staging).
Several disease conditions can be evaluated by NM imaging such as: Condylar hypoplasia, condylar hyperplasia, osteomyelitis, osteonecrosis, metabolic bone disorders (fibrous dysplasia, Paget’s disease, hyperparathyroidism), graft viability and oral cavity tumors.
Condylar hypoplasia: Condylar hypoplasia or aplasia is an abnormality caused by underdevelopment or non-development of the condyle. It can be congenial either unilateral or bilateral or acquired secondary to local (trauma, infection or irradiation) or due to systemic causes (toxic agents or rheumatoid arthritis) [1].
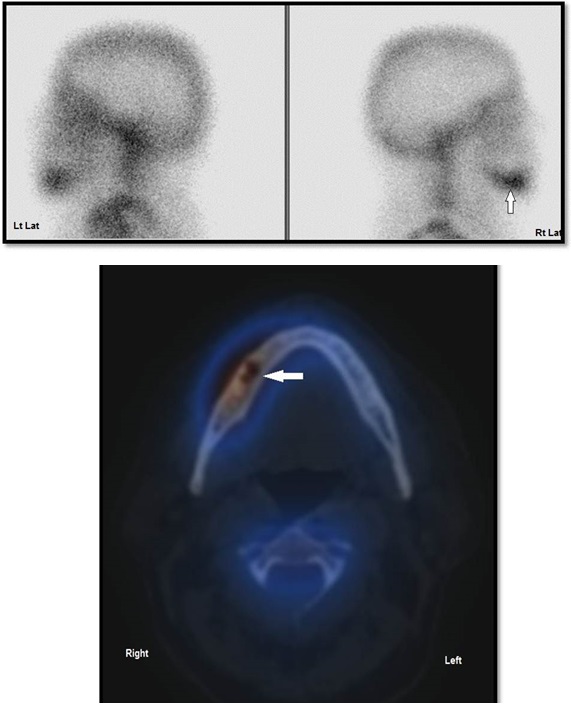
The diagnosis is usually by clinical examination, conventional radiographs, and 3dimensional CT. Bone scan is used to assess osteoplastic activity at initial diagnosis and on post -operative follow up of the affected condyle which appears underactive compared with the contralateral normal one. Figure 1 is a bone scan of a 21 year old female complaining of mandible deviation and right hypotrophic condyle since puberty, bone scan requested for confirmation and assess osteoplastic activity.
Bilateral aplasia is a congenital abnormality where both condyles are undeveloped and therefore underactive and are nonvisualized on SPECT/CT. Figure 2 is a bone scan of a 24-year-old female patient with bilateral hypoplasia of the mandibular condyles (Mandibulofacial dysostosis). Bone scan ordered to assess condyles osteoplastic activity.
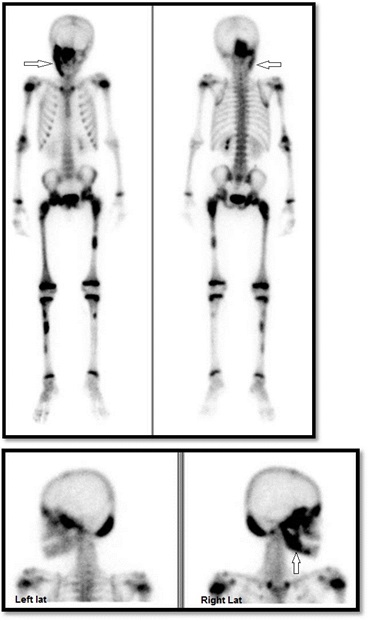
Condylar hyperplasia (CH): Condylar hyperplasia is a disorder characterized by overgrowth of the condyle. The main consequence of CH is unilateral facial asymmetry deformity, which combined with alteration of the dental occlusion with unilateral cross bite or open bite [2]. The disorder can present at any age and is more frequent in women [3]. Diagnosis of CH is based on clinical and radiographic findings [4]. Bone scan is used to assess condylar osteoplastic activity as base line and for follow up [5]. The affected site shows higher tracer uptake (overactive) on planar images (more than 10%) compared to the contralateral normal one [4]. SPECT CT has higher sensitivity than planar image with the added detection of structural changes. Figure 3 is a bone scan of a 23 years old male complaining of enlarged lower jaw in left temporomandibular area. Bone scan requested to assess osteoplastic condyles activity.
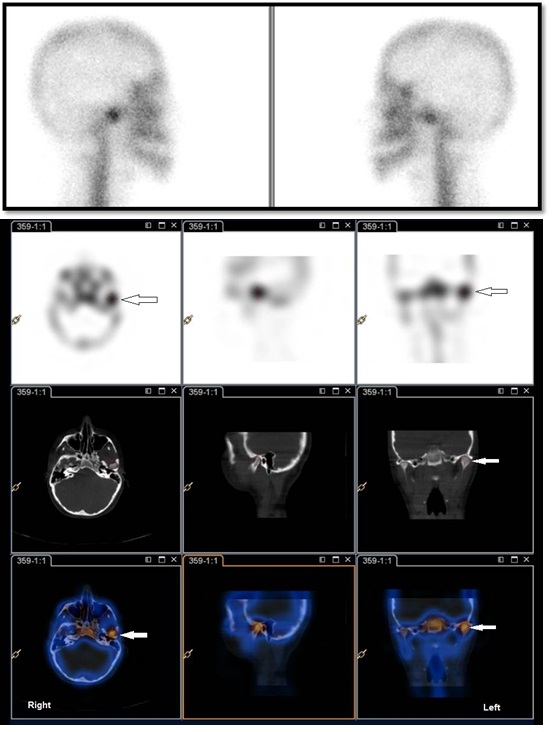
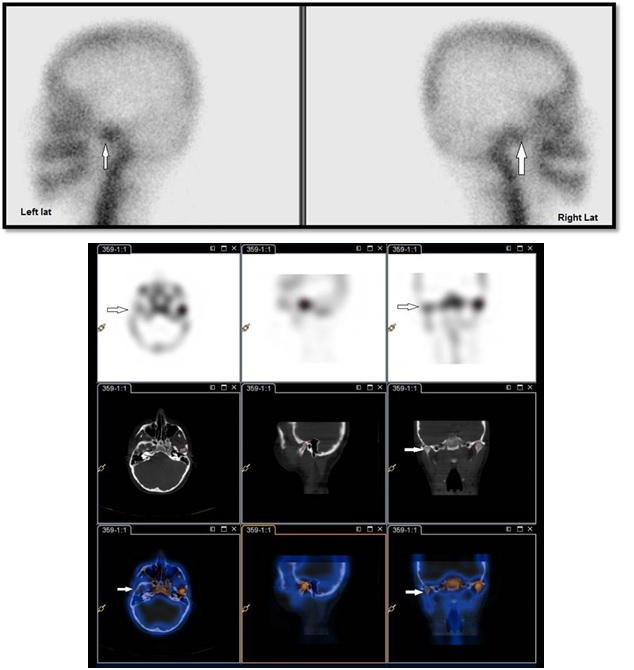
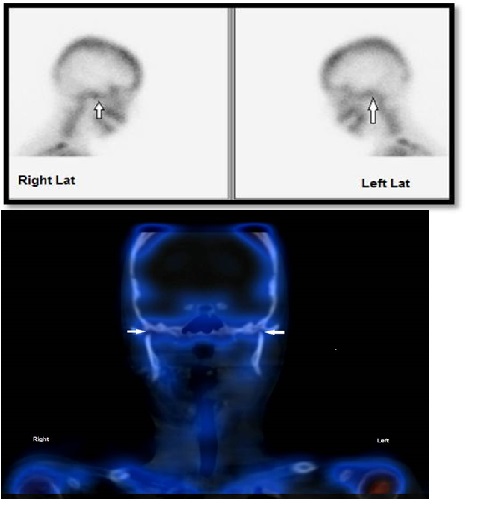
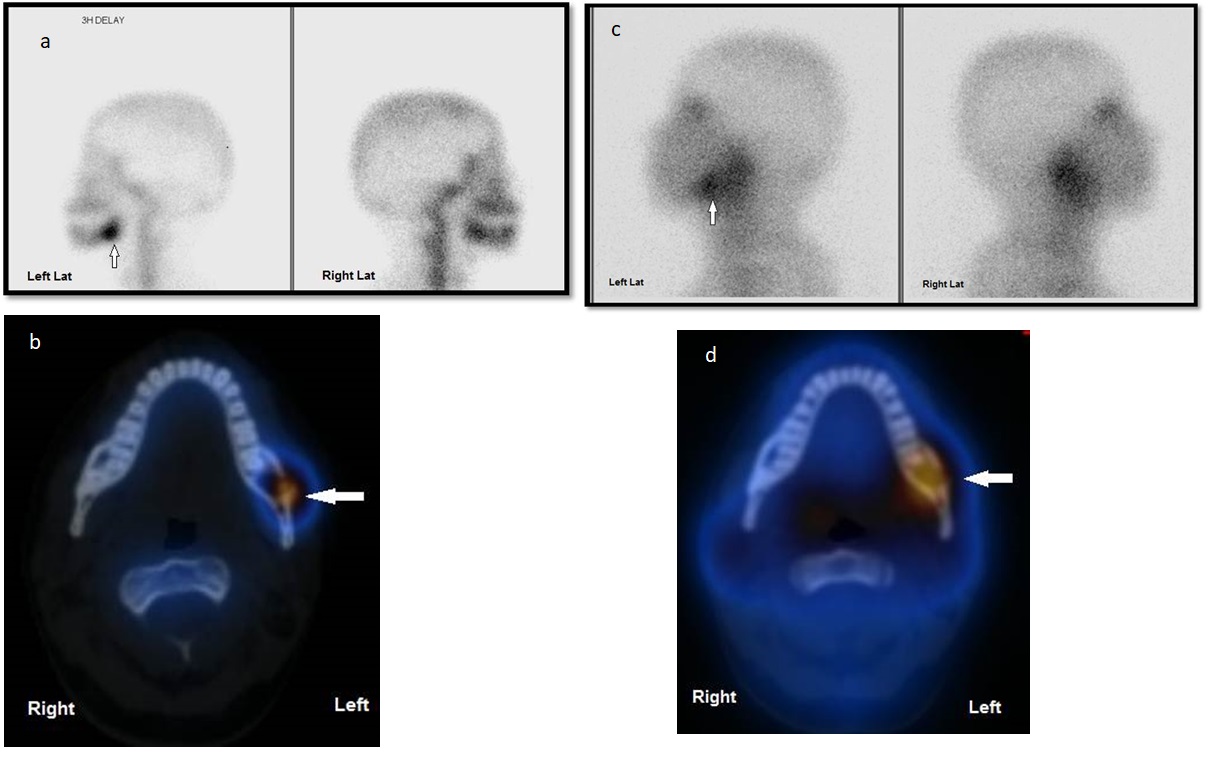
Osteomyelitis (OM): Osteomyelitis is an inflammatory condition of the bone marrow, which starts as an infection of the medullary cavity and extends thereafter to the haversian systems to involve the bony cortex and periosteum of the affected area [6]. OM of the jaws is mainly caused by spread of adjacent odontogenic infection. Several causes have been demonstrated, such as dentoalveolar infection, trauma, operative procedures, radiation, neoplasia, systemic bisphosphonate use, and genetic conditions [7,8]. Depending on clinical presentations, osteomyelitis is classified into acute, subacute and chronic [9]. The time of onset of symptoms is a key point to differentiate acute from chronic osteomyelitis while the former occurs within one month of the onset of symptoms the latter takes more than one month [10,11]. The signs and symptoms of chronic osteomyelitis probably less severe than those of an acute form, however most patients present with jaw pain, swelling and suppuration [12]. Diagnosis is usually based on history, clinical examination and radiology (panoramic x-ray, cone beam CT) and in some cases nuclear medicine studies are required to confirm diagnosis and monitor antibiotic therapy.
The NM criteria of active osteomyelitis of the jaw is matched increased uptake of tracer on both bone and gallium scan. Gallium scan is used to monitor therapy and once it’s normal indicate successful treatment. Bone scan is not useful to monitor therapy because it remains positive during repair healing phase. Figure 4 is a bone and gallium scan of a 26-year-old female patient presented with swelling on the left side of the lower jaw two weeks after tooth extraction. Bone and gallium scan ordered to rule out osteomyelitis.
Osteonecrosis of the jaw (ONJ): Osteonecrosis of the jaw, commonly called ONJ, occurs when blood supply to the jaw bone is interrupted and bone is exposed. Most cases of osteonecrosis of the jaw happen after a dental extraction. Other causes includes: Trauma, infection, steroid therapy, bisphosphonate used to treat osteoporosis and cancer therapy.
Diagnosis of ONJ is done when exposed, necrotic bone is present in the maxilla or mandible for at least 8 weeks. It may be asymptomatic for long period of time. When symptoms develop pain usually precedes other signs. In more advanced stage ONJ manifests with purulent discharge and pain from the exposed bone in the mandible and less likely from the maxilla. Imaging will help in confirming the diagnosis and monitor therapy. Plain radiograph may be diagnostic but more advanced imaging techniques may be ordered and include: cone beam CT, MRI, bone scan, and PET CT [13].
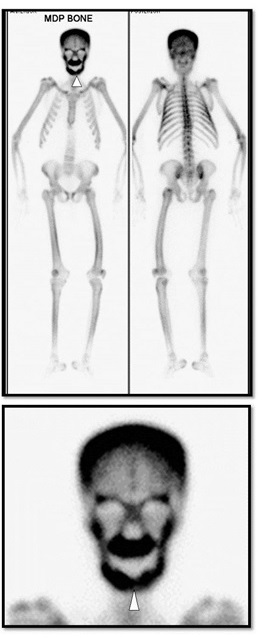
Figure 5 is a bone scan of a 68-year-old Saudi female patient with osteoporosis who developed pain in anterior right mandible two months after bisphosphonate therapy. Bone scan requested to rule out osteonecrosis of the jaw.
Fibrous dysplasia: Fibrous Dysplasia (FD) is a bone disorder in which normal bone and bone marrow are replaced by fibrous tissue [14]. There are three types of FD: monostotic, polyostotic, and polyostotic associated with endocrine disorders [15]. FD usually affect long bones, craniofacial bones, ribs, and pelvis [16]. Monostotic FD is less serious than polyostotic type however and because of high frequency in the jaws it is of greater concern to the dentist [17]. The diagnosis of FD is based on clinical examination and radiological examination (Panorama x-ray, cone beam CT, MRI, bone scan) and diagnosis confirmed by histopathologic examination. The general dentist can be the first to detect this disease in daily practice using panoramic radiography. Therefore, it is important for the dentist and oral surgeon to have good knowledge of FD in order to make the proper diagnosis and avoid complications of the disease. Bone scan shows marked increased uptake in the affected areas. Figure 6 is a bone scan of a 25-year-old female patient who presented to the dental clinic reporting a slow, painless increase in size of her right mandible over the last 6 years leading to facial deformity. A panoramic X-ray showed alteration in the pattern of the cancellous bone. Bone scan requested to assess extent and disease activity.
Hyperparathyroidism (HPT): HPT is a disorder characterized by increased Parathyroid Hormone (PTH) production by parathyroid glands. It can be primary HPT (parathyroid adenoma) or secondary HPT (due chronic renal failure). The PTH regulates serum calcium concentration and bone metabolism.
HPT affects women more than men in their fifth decade of life. Osteitis fibrosa cystica is the skeletal manifestation of primary HPT and can affect any bone including the jaws.
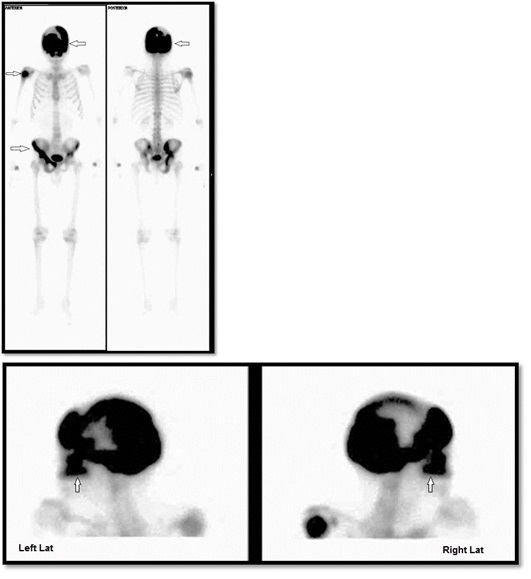
Diagnosis of HPT is mainly based on clinical and biochemical examination (Elevated serum PTH and hypercalcemia) and radiological examination including parathyroid nuclear scan and bone scan. The dentist and oral surgeon may suspect the diagnosis on panoramic radiograph or cone beam CT [18,19]. Bone scan will show the extent of the disease in whole the skeleton in general and facial bones in particular showing diffuse increased tracer uptake of the affected bones. Figure 7 is a bone scan of a 50-year-old female patient presented with progressive enlarging, painless swelling of the jaw with speech difficulty. The patient was diagnosed with primary hyperparathyroidism. Bone scan requested to assess extent and disease activity.
Paget’s disease (PD): Paget’s disease is a chronic progressive bone disease involving one bone (monostotic) or multiple bones (polyostotic) of the skeleton. It is characterized by rapid resorption and deposition of the affected bone, resulting in increased local vascularity and fibrous tissue in the marrow [20]. PD is a disease affecting both elderly male and female with age more than 50 year with male predominance and 3:2 ratio [21].
At early stage of the disease the patient may be asymptomatic. In more advanced stage the patient presents with pain and deformity of the affected bone. When the cranio-facial bones are involved (in particular the maxilla and/ or the mandible) facial deformity develops and the patient may complain of hearing and speaking difficulties [22].
The diagnosis of PD is based on clinical findings, radiological examinations including bone scan and elevated serum alkaline phosphatase. Whole body bone scan demonstrates disease extent with marked increased uptake in the affected areas in addition to its use for follow up and therapy monitoring.
Figure 8 is a bone scan of a 74-year-old male patient presented to the dentist reporting progressive swelling of the maxilla over the past few years. Panoramic x-ray showed cortical thickening of the body of the maxilla with teeth displacement. Bone scan requested to assess extent and disease activity.
PET CT: Squamous cell carcinoma (SCC) of the left maxilla
SCC of the oral cavity is a neoplastic process with certain risk factors mainly smoking and alcohol consumption. It can involve any part of the oral cavity. Usually it presents as a non-healing ulcer. In the early stages and patients will present with localized maxillary pain and teeth mobility.
Evaluation of mandibular and maxillary invasion in SCC is a major challenge to determine both therapeutic approach and prognosis [23]. Therefore, a reliable assessment is crucial for treatment planning to obtain both radical tumor resection and good functional results.
Different imaging modalities are used to assess mandibular and maxillary invasion by SCC of the oral cavity, including plain radiography, CT, thin cut 3 D mandibular and maxillary CT, MRI, bone scan, SPECT-CT, and PET/CT [24-28].
All of these modalities play certain roles in the evaluation of the mandible and maxilla, however each of them have specific pitfalls and therefore argument still exists about the optimal strategy in its use [26].
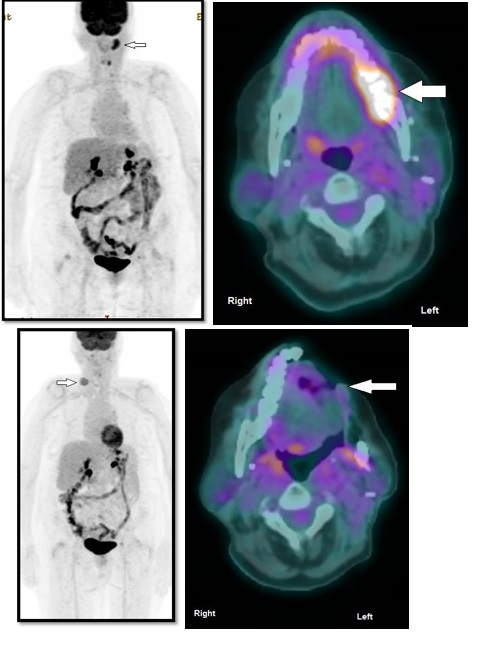
The reported sensitivities and specificities of CT, MR, and PET/CT appeared to be similar in the detection of mandibular and maxillary invasion by SCC of the oral cavity. The combined analysis of the 3 modalities yielded improved sensitivity compared with the single use of them without a statistically significant difference [29]. 18 F- PET/CT has the power to assess local extent of SCC, any distant metastases, post-operative and radiation therapy and evaluation for residual or recurrent disease. Figure 9 is a FDG PET/CT of a 40-year-old male patient with SCC of the mandible with jaw pain and limited mouth opening. FDG PET/CT was requested for initial staging and post-operative to assess therapy results.
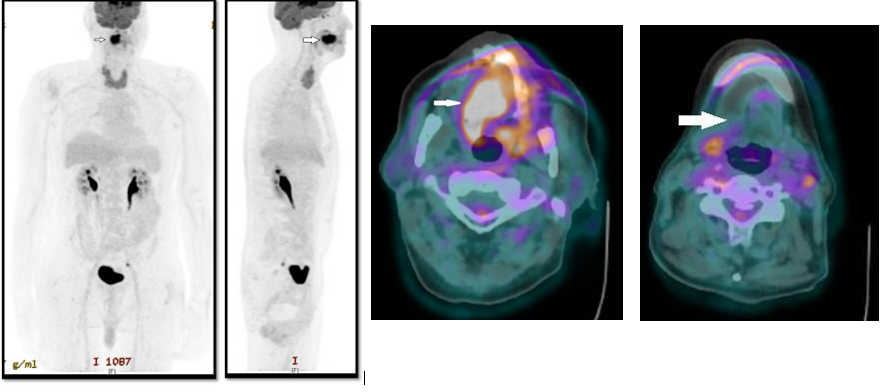
PET CT: Squamous cell carcinoma of the tongue: SCC of the tongue is one of the most common oral and maxillofacial malignant tumors [30]. Diagnosis is based on clinical, histological and radiological imaging. Studies have showed that CT and MRI provide morphological assessment of tongue cancer and unable to detect lymph node micro-metastasis. However, PET/CT provides both anatomical and metabolic information of tongue cancer and has several applications including staging, radiotherapy planning, treatment revision, response evaluation, and recurrence detection [31-33]. Figure 10 is a pre and postoperative FDG PET/CT of a 48-year-old male patient with SCC of the tongue.
Summary
Oro-facial pain is a common complaint in the dental and maxillofacial field. It can have a variety of causes, including infection, benign and malignant neoplasm, and metabolic diseases. Although oro-facial pain mostly is due to a local process, one should always rule out a systemic cause. This is especially true when no evident local lesion can be found. The diagnosis is usually based on clinical and radiological findings. However, when the treating physician still has some uncertainty in diagnosis or needs additional data, NM is a useful imaging tool offering important diagnostic information complementing the information obtained from other imaging modalities in particular a better understanding of the pathophysiology of the disease and therapy monitoring (Table 1).
Table 1:Indications and findings of nuclear odontology in different oral and dental disorders.
References
- Kaneyama K, Segami N, Hatta T. Congenital deformities and developmental abnormalities of the mandibular condyle in the temporomandibular joint. Congenit Anom (Kyoto). 2008; 48: 118-125.
- Hovell JH. Condylar hyperplasia. Br J Oral Surg. 1963; 1: 105-111.
- Nitzan DW, Katsnelson A, Bermanis I, Brin I, Casap N. The clinical characteristics of condylar hyperplasia: Experience with 61 patients. J Oral Maxillofac Surg. 2008; 66: 312-318.
- Saridin CP, Raijmakers PG, Tuinzing DB, Becking AG. Bone scintigraphy as a diagnostic method in unilateral hyperactivity of the mandibular condyles: a review and meta-analysis of the literature. Int J Oral Maxillofac Surg. 2011; 40: 11-17.
- Lewis EL, Dolwick MF, Abramowicz S, Reeder SL. Contemporary imaging of the temporomandibular joint. Dent Clin North Am. 2008; 52: 875-890.
- Topazian RG. Osteomyelitis of jaws. In: Topazian RG, Goldberg MH, editors. Oral and maxillofacial infections. 3rd ed. Philadelphia, PA: Saunders. 1994: 251-286.
- Koorbusch GF, Fotos P, Goll KT. Retrospective assessment of osteomyelitis. Etiology, demographics, risk factors, and management in 35 cases. Oral Surg OralMed Oral Pathol. 1992; 74: 149–154.
- Senel FC, Saracoglu Tekin U, Durmus A,Bagis B. Severe osteomyelitis of the mandible associated with the use of non-nitrogencontaining bisphosphonate (disodium clodronate): Report of a case. J Oral Maxillofac Surg. 2007; 65: 562–565.
- Yeoh SC, Mac Mahon S, Schifter M. Chronic suppurative osteomyelitis of the mandible: Case report. Aust Dent J. 2005; 50: 200-203.
- Marx RE. Chronic osteomyelitis of the jaws. Oral Maxillofac Surg Clin North Am. 1991; 3: 367.
- Mercuri LG. Acute osteomyelitis of the jaws. Oral Maxillofac Surg Clin North Am. 1991; 3: 355.
- Baltensperger M, Eyrich G. Osteomyelitis of the Jaws: definitions and classification. In: Baltensperger M, Eyrich G, editors. Osteomyelitis of jaws. Berlin: Springer. 2009; 5-56.
- Khan A, Morrison A, Cheung A, et al: Osteonecrosis of the jaw (ONJ): Diagnosis and management in 2015. Osteoporos Int. 2016; 27: 853-859.
- Lichtenstein L. Polyostotic fibrous dysplasia. Arch Surg. 1938; 36: 874-898.
- DiCaprio MR, Enneking WF. Fibrous dysplasia. Pathophysiology, evaluation, and treatment. J Bone Joint Surg Am. 2005; 87: 1848-1864.
- Ogunsalu C, Smith NJ, Lewis A. Fibrous dysplasia of the jaw bone: A review of 15 new cases and two cases of recurrence in Jamaica together with a case report. Aust Dent J. 1998; 43: 390–394.
- Marx SJ. Hyperparathyroid and hypoparathyroid disorders. N Engl J Med. 2000; 343: 1863-1875.
- Kakade SP, Gogri AA, Umarji HR, Kadam SG. Oral manifestations of secondary hyperparathyroidism: A case report. Contemp Clin Dent. 2015; 6: 552-558.
- Kanis JA. Editor Pathophysiology and treatment of Paget’s diseases of bone. 2nd ed. London: Martin Dunitz. 1998.
- Joshi SR, Ambhore S, Butala N, Patwardhan M, Kulkarni M, Pai B, et al. Paget’s disease from western India. J Assoc Physicians India. 2006; 54: 535-538.
- Fredrick R, Singer CH. Paget’s disease of bone. Bone program. Santa Monica, California: A Publication of the Paget Foundation for Paget’s Disease of Bone and Related Disorders. 2008.
- Llewellyn CD, Johnson NW, Warnakulasuriya KA. Risk factors for squamous cell carcinoma of the oral cavity in young people— a comprehensive literature review. Oral Oncol. 2001; 37: 401– 418.
- Brown JS, Griffi th JF, Phelps PD, Browne RM. A comparison of different imaging modalities and direct inspection after periosteal stripping in predicting the invasion of the mandible by oral squamous cell carcinoma. Br J Oral Maxillofac Surg. 1994; 32: 347-359.
- van den Brekel MW, Runne RW, Smeele LE, Tiwari RM Snow GB, Castelijns JA. Assessment of tumour invasion into the mandible: the value of different imaging techniques. Eur Radiol. 1998; 8: 1552-1557.
- Close LG, Merkel M, Burns DK, Schaefer SD. Computed tomography in the assessment of mandibular invasion by intraoral carcinoma. Ann Otol Rhinol Laryngol. 1986; 95: 383-388.
- Bahadur S. Mandibular involvement in oral cancer. J Laryngol Otol. 1990; 104: 968-971.
- Tsue TT, McCulloch TM, Girod DA, Couper DJ, Weymuller EA, Glenn MG. Predictors of carcinomatous invasion of the mandible. Head Neck. 1994; 16: 116-126.
- Brown JS, Lewis-Jones H. Evidence for imaging the mandible in the management of oral squamous cell carcinoma: a review. Br J Oral Maxillofac Surg. 2001; 39: 411-418.
- Dong Hyeon Gu, Dae Young Yoon, Chan Hee Park, Suk Ki Chang, Kyoung Ja Lim, Young Lan Seo, Eun Joo Yun, Chul Soon Choi & Sang Hoon Bae. CT, MR, 18FFDG PET/CT, and their combined use for the assessment of mandibular invasion by squamous cell carcinomas of the oral cavity, Acta Radiologica. 2010; 51: 1111- 1119.
- Rui-Pionheiro A, Jose LL, Enrique JS, Jorge RS and Carlos I. A pioneering epidemiological study investigating the incidence of squamous cell carcinoma of tongue in a Portuguese population. Med Oral Patol Oral Cir Buca. 2012; 17: e550-e554.
- Troost EG, Schinagl DA, Bussink J, Oyen WJ and Kaanders JH. Clinical evidence on PET-CT for radiation therapy planning in head and neck tumours. Radiother Oncol. 2010; 96: 328-334.
- Schwartz DL, Macapinla HA and Weber RS.FDGPET staging of head and neck cancer-can improved imaging lead to improved treatment. J Natl Cancer Inst. 2008; 100: 688-689.
- Bussink J, Van Herpen CM, Kaanders JH and Oyen WJ. PET-CT for response assessment and treatment adaptation in head and neck cancer.Lancet Oncol. 2010; 11: 661-669.