
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Attenuation of CALCR protein expression in stone affected region of kidney biopsy tissue: Case presentation
Pubali Mitra1; Dilip Kumar Pal2; Madhusudan Das1*
1Department of Zoology, University of Calcutta, 35 Ballygunge Circular Road, Kolkata 700019, West Bengal, India.
2 Department of Urology, Institute of Post Graduate Medical Education & Research, 244 A.J.C Bose Road, Kolkata 700020, West Bengal, India.
*Corresponding Author : Madhusudan Das
Department of Zoology, University of Calcutta, 35
Ballygunge Circular Road, Kolkata 700019, West
Bengal, India.
Email: madhuzoo@yahoo.com
Received : Mar 29, 2021
Accepted : Apr 28, 2021
Published : Apr 30, 2021
Archived : www.jcimcr.org
Copyright : © Das M (2021).
Abstract
Calcitonin is one of the most important hormones in human body which regulates calcium homeostasis. It binds with Calcitonin Receptor (CALCR) and reduces serum calcium level by inhibiting bone resorption and proximal renal reabsorption. Alteration in calcium homeostasis promotes diseases like osteoporosis, urolithiasis etc. An interesting finding of reduced CALCR protein expression in a urolithiasis patient motivated us to investigate its level in stone affected region of kidney biopsy tissue and hence in the present study, CALCR expression was checked in urolithiasis patients who had gone through open nephrolithotomy for stone removal. Basic and clinical parameters of the patients were recorded followed by analysis of stone composition, genotypic analysis and studying CALCR protein expression level in the kidney biopsy tissue samples (in the location of stone and an adjacent control area). CALCR protein expression was found to be attenuated in the stone affected region of kidney biopsy tissue as compared to adjacent control tissues (4-6 cm apart from the stone affected region) in all our studied samples (n=5). This case series represents an interesting finding as it is the first time report in the world, regarding expression of CALCR protein in kidney tissues of urolithiasis patients.
Keywords: Urolithiasis; CALCR; Protein expression; SNP.
Abbreviations: CALCR: Calcitonin Receptor; SNP: Single Nucleotide Polymorphism; Ser: Serine; Pro: Proline; Leu: Leucine; UTR: Untranslated Region; BMI: Body Mass Index; FT-IR Spectroscopy: Fourier Transform Infrared Spectroscopy; KBr: Potassium Bromide; EDTA: Ethylene Diamine Tetraacetic Acid; PCR: Polymerase Chain Reaction; MgCl2 : Magnesium Chloride; DNTP: Deoxynucleotide Triphosphates; DAB: Diaminobenzidine; NaCl: Sodium Chloride; Na3 VO4 : Trisodium Tetraoxovanadate; SDS-PAGE: Sodium Dodecyl Sulfate- Polyacrylamide Gel Electrophoresis; TBST: TRIS Buffered Saline; ESWL: Extracorporeal Shock Wave Lithotripsy; PCNL: Percutaneous Nephrolithotomy.
Citation: Mitra P, Pal DK, Das M. Attenuation of CALCR protein expression in stone affected region of kidney biopsy tissue: Case presentation. J Clin Images Med Case Rep. 2021; 2(2): 1088.
Background
Urolithiasis is one of the most common clinical problems worldwide, which is a rising concern and a major economic burden on healthcare system. It involves formation of stone by successive events of supersaturation, nucleation, aggregation and finally retention [1] of stone forming crystals in kidney or ureter or urinary bladder of human urinary system. The disease occurs in all parts of the world and affects about 12% of the world population [2]. It causes intense colicky pain in the back, flank, lower abdomen and groin region, brings about significant morbidity including hematuria, urinary tract infection, hydronephrosis, decreased renal function and sometimes in bilateral cases, renal failure.
In Asia, about 1-19.1% of individuals suffer from urolithiasis in lifetime. India falls under the stone forming belt of Asia [3], where the prevalence of kidney stones is 15% and approximately 5 to 7 million patients are suffering from urolithiasis. Its occurrence is high in the northern, north western and central part of India. In West Bengal, the scenario also indicates that urolithiasis poses a major health hazard in both rural and urban societies. Prevalence of the disease has increased over the past few decades and both extrinsic and intrinsic factors promote chances of kidney stone formation. Environmental exposure, climatic variation, water intake, dietary habit, obesity, stress, sedentary lifestyle of an individual are the external factors and age, gender, race, ethnicity and genetic perspective of an individual are the most common intrinsic factors that drive kidney stone formation [4,5].
Several studies reported association of genes and genetic polymorphisms with urolithiasis in different ethnic populations of the world. The calcitonin receptor protein encoding Calcitonin Receptor CALCR gene polymorphisms were found to be associated with urolithiasis in the Taiwan [6] and Indian population [7,8], which seems to be useful markers for the susceptibility of the disease. Our previous work has revealed significant association of CALCR gene polymorphisms with kidney stone risk in our study population of West Bengal [8]. However, there is no prior report whether the protein expression alters in urolithiasis patients. In the present study we have focused to check the CALCR protein expression level in the stone affected region of kidney biopsy tissue as compared to adjacent control tissues in urolithiasis patients.
Case presentation
In our four year (July, 2016- June, 2020) study with 278 urolithiasis patients, five patients (n=5) had to undergo open nephrolithotomy for removal of stone. Their detailed information like gender, age, BMI, place of living, lifestyle, food habit, fluid intake habit, history of renal stone episodes and family history of renal stone were collected from the study participants through a questionnaire. Serum sample was collected to analyse concentrations of calcium, urea and creatinine. Urinary concentrations of calcium, oxalate, potassium, citrate, phosphate and urate were quantified by standard techniques from urine collected over a period of 24 hour. Stone composition was analysed by FT-IR (Fourier Transform Infrared) spectroscopy. Genotypic analysis for CALCR was performed using genomic DNA extracted from peripheral blood samples followed by DNA amplification using specific primers (Table 1) and then bi-directional DNA sequencing and analysis. From each patient, two biopsy tissue samples were retrieved by physicians, one from the part of kidney which was in contact with the stone and the other from the control area (4-6 cm away from the stone area). It was confirmed by the physician that the control area was free from the Randall’s plaque. One part of surgically excised tissue samples were fixed in Bouin’s fluid fixative in room temperature and processed to embed in paraffin for immunohistochemical study of the protein. The other part was kept in -20°C refrigerator and following standard techniques immunoblotting was performed.
Table 1: Primer sequences used for detection of CALCR gene polymorphisms.
SNP |
Location |
Primers (5’ – 3’) |
Amplicon length |
Annealing temperature |
rs2301680 |
Exon 4 |
F: GAGGGCCTCAGGTATAACAATC |
509 bp |
64º C |
rs1801197 |
Exon 13 |
F: TTTCTCTTCCAGGTCCAAACC |
766 bp |
64º C |
rs1042138 |
3’ UTR |
The basic and clinical characteristics of the five patients and genotypes for the three SNPs (rs2301680, rs1801197 and rs1042138) of CALCR gene are presented in Table 2. Recurrence of stone episodes was observed in three patients. It was found that calcium oxalate was the major constituent of kidney stone in all the five patients studied.
Table 2: Basic and clinical characteristics of urolithiasis patients of the study group.
Patient ID |
K66-A |
K80-B |
K124-C |
K191-D |
K233-E |
|
Age |
62 |
42 |
48 |
34 |
50 |
|
Gender |
Male |
Female |
Male |
Male |
Male |
|
BMI |
23.5 kg/m2 |
22.8 kg/m2 |
21.6 kg/m2 |
26.0 kg/m2 |
23.4 kg/m2 |
|
Lifestyle |
Non-sedentary |
Non-sedentary |
Non-sedentary |
Non-sedentary |
Sedentary |
|
Food habit |
Non-vegetarian |
Vegetarian |
Non-vegetarian |
Non-vegetarian |
Non-vegetarian |
|
Stone episodes (Years) |
2008, 2011, 2016, 2018 |
- |
2012, 2017 |
2013, 2015, 2016 |
- |
|
Stone composition |
Calcium oxalate monohydrate, protein and anhydrous uric acid |
Calcium oxalate |
Calcium oxalate monohydrate, ammonium urate, and carbonate apatite |
Calcium oxalate, Calcium phosphate, ammonium, urate and anhydrous uric acid |
Calcium oxalate |
|
Stone size |
2.4cm x 1.8cm |
3.86cm x 2.0cm |
2.4cm x 2.3 cm |
3.1cm x 1.9cm |
4.2cm x 3.6cm |
|
Stone weight |
3.31 gm |
5.91 gm |
2.89 gm |
5.24 gm |
8.54 gm |
|
Clinical parameters |
Serum calcium |
9.02 mg/dL |
9.24 mg/dL |
9.12 mg/dL |
8.90 mg/dL |
9.00 mg/dL |
|
Urinary calcium |
6.26 mmol/24h |
4.86 mmol/24h |
6.18 mmol/24h |
7.26 mmol/24h |
5.94 mmol/24h |
|
Urinary oxalate |
28.04 mg/24h |
24.28mg/24h |
37.46 mg/24h |
31.52 mg/24h |
20.46 mg/24h |
|
Urinary citrate |
2.7 mmol/24h |
1.85 mmol/24h |
4.06 mmol/24h |
2.68 mmol/24h |
3.24 mmol/24h |
|
Urinary phosphate |
27.58 mmol/24h |
15.62 mmol/24h |
34 mmol/24h |
24.46 mmol/24h |
22.88 mmol/24h |
|
Urinary potassium |
65 mmol/24h |
34.2 mmol/24h |
44.4 mmol/24h |
42.6 mmol/24h |
29 mmol/24h |
|
Urinary urate |
2.8 mmol/24h |
2.6 mmol/24h |
1.9 mmol/24h |
2.7 mmol/24h |
3.0 mmol/24h |
|
Fasting Urinary pH |
5.76 |
5.2 |
5.36 |
4.02 |
4.94 |
CALCR SNP |
rs2301680 (Ser17Pro) |
TT genotype (wild) |
TC genotype (heterozygous) |
TT genotype (wild) |
TC genotype (heterozygous) |
TC genotype (heterozygous) |
rs1801197 (Leu447Pro) |
TT genotype (variant) |
TT genotype (variant) |
CT genotype (heterozygous) |
CT genotype (heterozygous) |
TT genotype (variant) |
|
rs1042138 (3’ UTR) |
TT genotype (variant) |
CT genotype (heterozygous) |
CT genotype (heterozygous) |
TT genotype (variant) |
CT genotype (heterozygous) |
|
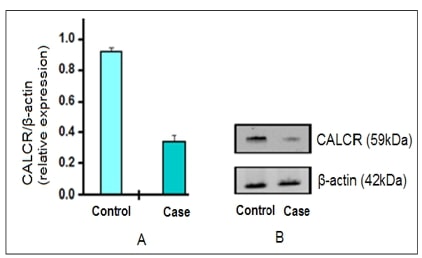
The protein expression study revealed attenuation in the CALCR protein expression level in the stone affected region of kidney biopsy tissue as compared to adjacent control tissues and this was evident from immunohistochemistry (Figure 1) and further validated by immunoblot (Figure 2) result. Rabbit polyclonal anti-CALCR (ab11042) was used as primary antibody. (Figure 1A) is the negative control of immunohistochemistry study where no primary antibody was used. Immunohistochemistry staining for CALCR was detected as brown stain in the control as well as case tissue. The immunostaining was found to be attenuated in case sample (Figure 1C) as compared to adjacent control (Figure 1B) tissue. In order to confirm the immunohistochemistry result, biopsy tissue samples were subjected to SDS-PAGE followed by western blot, keeping β-actin as the loading control. The immunoblot analysis also showed decline of CALCR protein expression level in the case samples as compared to adjacent controls (Figure 2).

Discussion
Urolithiasis is a globally common clinical problem that involves stone formation in urinary tract by supersaturation of urine. A supersaturated urine with concentration above formation product is unstable and then crystals form in any of the three parts (kidney, ureter, and urinary bladder) of urinary tract. As hypercalciuria is the major risk factor in kidney stone formation, the study of calcium homeostasis regulating genes and encoded proteins seems to be important. In response to elevated serum calcium levels, the polypeptide hormone calcitonin secretes from parafollicular cells of thyroid gland and reduces serum calcium level by inhibiting bone resorption, proximal renal reabsorption and thus enhancing urinary calcium excretion [9,10]. This calcitonin activity is mediated by calcitonin receptors (CALCR) which are proteins of class B of the seven pass transmembrane domain G-protein coupled receptor superfamily. CALCR protein expression has been reported in various adult tissues like kidney, osteoclast, prostate, placenta, skeletal muscle etc [11]. In postnatal rat kidney, the expression of calcitonin receptor protein was reported to be evident in distal convoluted tubules, thick ascending limb of loop of henle and collecting ducts.
As there is no prior report on expression study of CALCR protein in kidney tissues of urolithiasis patients, here in the present study we have attempted to check the intensity of CALCR expression in stone affected region of urolithiasis patients and adjacent control tissues. Now-a-days, urolithiasis patients are mostly treated with minimally invasive techniques like ESWL, PCNL etc and only 2% of kidney stones require open surgery. Open surgeries are practised in cases of patients with recurrent stone episodes, patients with complex stone burden, with anatomical anomalies or with comorbidities [12]. In this study, five patients have undergone open nephrolithotomy, where ancillary procedure like pyeloplasty was required along with stone surgery and in cases of large staghorn calculus. We have checked CALCR protein expression in kidney biopsy tissue samples of those five patients and the result showed attenuation in stone affected region as compared to adjacent control tissues.
As the physiological effect of calcitonin on kidney is to increase calcium excretion by inhibiting renal tubular calcium resorption [13] and this effect is mediated by the high affinity Calcitonin Receptor (CALCR), hence attenuation of CALCR expression in biopsy kidney tissue sample of urolithiasis patients seems to be of great interest. However, our preliminary result needs to be validated with larger sample size.
Declaration
Ethics approval and consent to participate: This study was approved by the Institutional Ethics Committee [Memo No. INST/IEC/2016/374 dated 06.06.2016] of Institute of Post Graduate Medical Education & Research (IPGME & R), Kolkata, West Bengal, India. Written informed consent was obtained from each study participant included in the study.
Competing interests: The authors declare no conflict of interest and do not have anything to disclose.
Funding: Department of Science and Technology (DST), Government of India (Ref. No. DST/INSPIRE Fellowship/2016/ IF160107, awarded to Pubali Mitra).
Authors' contributions: PM and MD conceptualized and designed the study; PM performed the experiments; PM analyzed the data; MD contributed reagents/materials/analysis tools; DKP provided blood and kidney biopsy tissue samples along with clinical data; PM drafted the manuscript with important intellectual inputs from DKP; MD critically revised the manuscript and supervised the entire work. All authors have read and approved the manuscript.
Acknowledgements: The authors would like to acknowledge the study participants who gave their consent and collaborated in this study and Dr. Subir Dutta of Scientific Clinical Research Laboratory Pvt. Ltd. Kolkata for assistance in serum and urinary calcium testing.
References
- Mandel N. Mechanism of stone formation. Semin Nephrol. 1996; 16: 5.
- Alelign T, Petros B. Kidney stone disease: an update on current concepts. Adv Urol 2018; ID 3068365.
- Lopez M, Hoppe B. History, epidemiology and regional diversities of urolithiasis. Pediatr Nephrol. 2010; 25: 1.
- Curhan GC, Willett WC, Rimm EB, Stampfer MJ. Family history and risk of kidney stones. J Am Soc Nephrol. 1997; 8: 10.
- Shakhssalim N, Basiri A, Houshmand M, Pakmanesh H, Golestan B, Azadvari M, Aryan H, Kashi AH. Genetic polymorphisms in calcitonin receptor gene and risk for recurrent kidney calcium stone disease. Urol Int 2014; 92: 3.
- Chen WC, Wu HC, Lu HF, Chen HY, Tsai FJ. Calcitonin receptor gene polymorphism: a possible genetic marker for patients with calcium oxalate stones. Eur Urol. 2001; 39: 6.
- Bid HK, Chaudhary H, Mittal RD. Association of vitamin-D and calcitonin receptor gene polymorphism in paediatric nephrolithiasis. Pediatr Nephrol. 2005; 20: 6.
- Mitra P, Guha M, Ghosh S, Mukherjee S, Bankura B, Pal DK, Maity B, Das M. Association of calcitonin receptor gene (CALCR) polymorphism with kidney stone disease in the population of West Bengal, India. Gene 2017; 622.
- Bushinsky DA, Monk RD. Electrolyte quintet: Calcium. Lancet. 1998; 352: 9124.
- Masi L, Brandi ML. Calcitonin and calcitonin receptors. Clin Cases Miner Bone Metab. 2007; 4: 2.
- Tikellis C, Xuereb L, Casley D, Brasier G, Cooper ME, Wookey PJ. Calcitonin receptor isoforms expressed in the developing rat kidney. Kidney Int. 2003; 63: 2.
- Cakici OU, Ener K, Keske M, Altinova S, Canda AE, Aldemir M, Ardicoglu A. Open stone surgery: A still-in-use approach for complex stone burden. Cent European J Urol. 2017; 70: 2.
- Pondel M. Calcitonin and calcitonin receptors: Bone and beyond. Int J Exp Pathol. 2000; 81: 6.