
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Air bubble after intrathecal triamcinolone acetonide application in a progressive multiple sclerosis patient
Thomas Müller*; Sven Lütge; Gunnar Gäde
Department of Neurology, St. Joseph Hospital Berlin-Weissensee, Gartenstr. 1, 13088 Berlin, Germany
*Corresponding Author : Thomas Müller
Department of Neurology, St. Joseph Hospital BerlinWeißensee, Gartenstr. 1, 13088 Berlin, Germany.
Email: th.mueller@alexius.de &
thomas.mueller@ruhr-uni-bochum.de
Received : Mar 30, 2021
Accepted : Apr 28, 2021
Published : Apr 30, 2021
Archived : www.jcimcr.org
Copyright : © Müller T (2021).
Keywords: Triamcinolon; Multiple sclerosis; Air bubble.
Citation: Müller T, Lütge S, Gäde G. Air bubble after intrathecal triamcinolone acetonide application in a progressive multiple sclerosis patient. J Clin Images Med Case Rep. 2021; 2(2): 1090.
Case presentation
Repeated intrathecal application of the sustained release steroid Triamcinolone Acetonide (TCA) is beneficial in progressive Multiple Sclerosis (MS) patients [1]. Particularly, patients with spinal lesions often show a distinct benefit with a three fold increase of the maximum walking distance [2]. This therapy ameliorates walking distance, improves upper limb function and reduces spastic symptoms [1]. The putative regenerative effect may result from declined synthesis of the repulsive guidance molecule A [3]. Visualization of air bubbles after a TCA injection prompted this case report.
The female patient was diagnosed with primary progressive MS eleven years ago. T2 weighted Magnetic Resonance Imaging (MRI) scans showed typical lesions, located in periventricular, iuxtacortical, infratentorial areas and in the spinal cord. P100 latencies of visual evoked potentials were prolonged on both sides. She suffered from right accentuated paraspastis of the lower limbs with a maximum of walking distance of 300 meters. TCA treatment was initiated. One day after the second lumbar 40 mg TCA containing injection, we incidentally performed a cranial 1.5 TESLA MRI scan (Siemens) as a routine follow up examination, done at least one time per year. We found in the region of the right frontal lobe (Figures 1 & 2) an air bubble, visualized with the T2 weighted MRI images. It resulted from the TCA injection, when TCA was aseptically dissolved in 9% NaCl isotonic physiological solution without bubble removal accidentally before the application. The patient did not experience any side effects. There were no clinical signs of acute inflammatory reactions. Control of cerebrospinal fluid showed no abnormalities two days later.
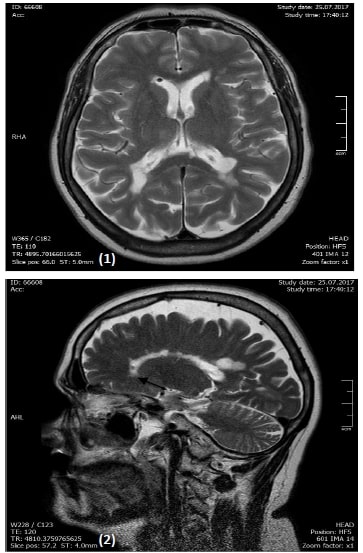
In MRI, different materials are visible in the image, as they have different proton densities and relaxation times. The presence of different materials in the sample being imaged can cause additional image artefacts. Cerebrospinal fluid and air have different magnetic susceptibilities [4]. The local magnetic field strength near a susceptibility boundary will be altered by the field induced in cerebrospinal fluid and air. This in turn will affect both the MRI signal and the imaging method [4]. In this case, the air bubble caused a magnetic field inhomogeneity [4]. It reduced T2 and caused a weaker signal as dark image for gradient-echo images. The inhomogeneous magnetic field interferes with the mapping between physical location and image pixels [5]. This occurs because the methods used to distinguish signals from spins at different locations work on the assumption of a perfectly homogenous magnetic field [5]. The presence of an additional dipole field means the protons experience a different magnetic field strength to the one they would feel in a perfectly homogenous field, and as a result process at a different frequency [5]. Thus any position encoding which relates frequency to position will wrongly register the position of the proton. Although too noisy with a too low resolution, there was also a detectable arrowhead shape (Figure 1) [4,5]. In this case, missing bubble removal from the TCA containing syringe had no serious clinical consequences. Nevertheless we recommend that bubbles in the TCA solution should be avoided before intrathecal application. The patient responded in the further course with increased maximum walking distance to 400 meters [1,6].
References
- Muller T. Role of intraspinal steroid application in patients with multiple sclerosis. Expert Rev Neurother. 2009; 9: 1279-12787.
- Lukas C, Bellenberg B, Hahn HK, Rexilius J, Drescher R, et al. Benefit of repetitive intrathecal triamcinolone acetonide therapy in predominantly spinal multiple sclerosis: prediction by upper spinal cord atrophy. Ther Adv Neurol Disord. 2009; 2: 42-49.
- Muller T, Barghorn S, Lutge S, Haas T, Mueller R, et al. Decreased levels of repulsive guidance molecule A in association with beneficial effects of repeated intrathecal triamcinolone acetonide application in progressive multiple sclerosis patients. J Neural Transm (Vienna) 2015; 122: 841-848.
- Weisskoff RM, Zuo CS, Boxerman JL, Rosen BR. Microscopic susceptibility variation and transverse relaxation: Theory and experiment. Magn Reson Med. 1994; 31: 601-610.
- Hardy P, Henkelman RM. On the transverse relaxation rate enhancement induced by diffusion of spins through inhomogeneous fields. Magn Reson Med. 1991; 17: 348-356.
- Hoffmann V, Schimrigk S, Islamova S, Hellwig K, Lukas C, Brune N, et al. Efficacy and safety of repeated intrathecal triamcinolone acetonide application in progressive multiple sclerosis patients. J Neurol Sci. 2003; 211: 81-84.