
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A delayed acute complication: Gastric remnant hemorrhagic ulcer after mini-gastric bypass
Hasan Maden1*; Mustafa Şahin2; Akın Çalışır2; Enes Şahin3
1 Department of General Surgery, Ordu Gölköy Public Hospital, Turkey.
2 Department of General Surgery, Selçuk University Hospital, Turkey.
3 Department of General Surgery, Kocaeli Public Hospital, Turkey.
*Corresponding Author : Hasan Maden
Department of General Surgery, Ordu Gölköy Public
Hospital, Turkey.
Email: hasanmaden@gmail.com
Received : Apr 01, 2021
Accepted : Apr 28, 2021
Published : Apr 30, 2021
Archived : www.jcimcr.org
Copyright : © Maden H (2021).
Abstract
Mini-gastric bypass is a common procedure for bariatric surgery. This procedure creates and excluded gastric remnant and this part can’t be accessed easily. Some complications of this gastric remnant has been reported but there is not a reported case of acute bleeding from there. Our report presents and 37 year old woman who had undergone bariatric surgery 6 years ago. Mini-gastric bypass was performed to this patient. The patient comes to the emergency service with signs of upper gastrointestinal bleeding. After hospitalization, examinations showed us that the patient was bleeding from the remnant stomach. The remnant stomach and the first part of the duodenum were resected with laparoscopic surgery. At 6 months followup, the patient has had no further episodes of gastrointestinal hemorrhage.
Keywords: Gastric remnant; Hemorrhagic ulcer; Mini-gastric bypass; Red blood cell scintigraphy.
Citation: Maden H, Şahin M, Çalişir A, Şahin E. A delayed acute complication: Gastric remnant hemorrhagic ulcer after mini-gastric bypass. J Clin Images Med Case Rep. 2021; 2(2): 1095.
Introduction
The Roux-en-Y Gastric Bypass (RYGB) and sleeve gastrectomy are the most commonly worldwide-performed procedures in current practice of bariatric surgery [1-3]. Despite the popularity of RYGB, a new concept of gastric bypass has emerged as a new alternative and the Mini-Gastric Bypass (MGB) has become an increasingly prevalent bariatric surgical procedure across the globe, and represented 1.5% of all surgeries performed [2]. In both gastric bypass surgeries, after the closure of the upper part of the stomach, a jejunal reconstruction is performed. This configuration creates an excluded gastric remnant in abdomen. The most important drawback of gastric bypass surgeries is inaccessibility of the excluded stomach. The diagnosis and treatment of developing diseases in the excluded stomach are challenging limitations [4]. After RYGB, some rare delayed acute complications such as perforation and bleeding of the biliopancreatic limb and the excluded stomach have been reported [5]. However, there is not a reported case of acute gastric remnant bleeding complication after MGB.
This report describes the case of a 37-year-old patient, presented in an emergency setting with a bleeding from duodenal ulcer six years after MGB.
Case report
A 37-year-old woman who had undergone laparoscopic MGB in 2014 presented to emergency department complaining of weakness, mild epigastrik pain and melena. Six weeks before the current hemorrhagic episode, the patient reported intermittent emission of melanic stools and epigastrik pain, for which she was admitted to a local hospital. Laboratory findings revealed a hemoglobin level of 6.1 g/dL and iron deficiency. Endoscopy and abdominal computed tomography was performed and no abnormalities apart from anatomical changes related to surgery was found. She was discharged asymptomatic 48 hour later with iron supplement prescribe.
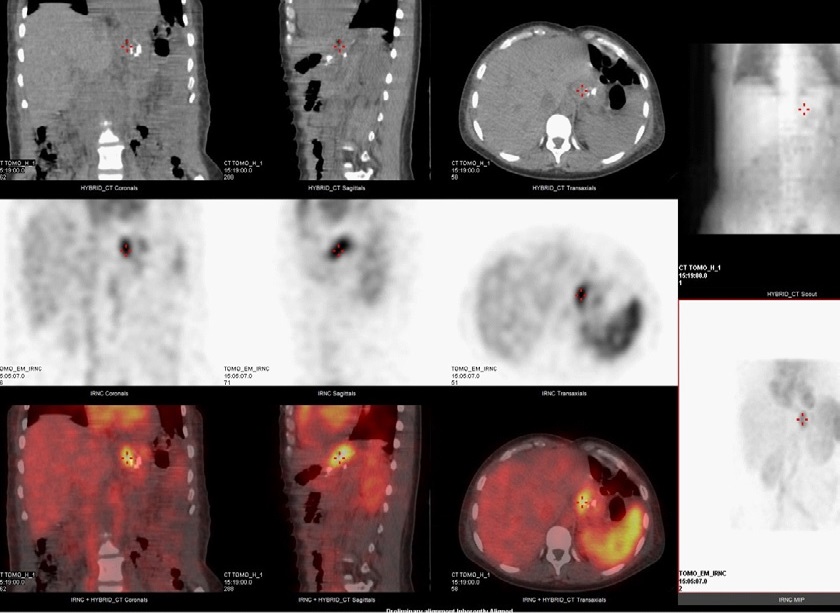
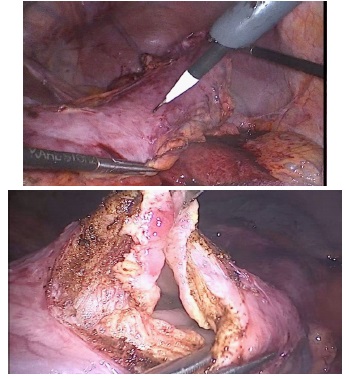
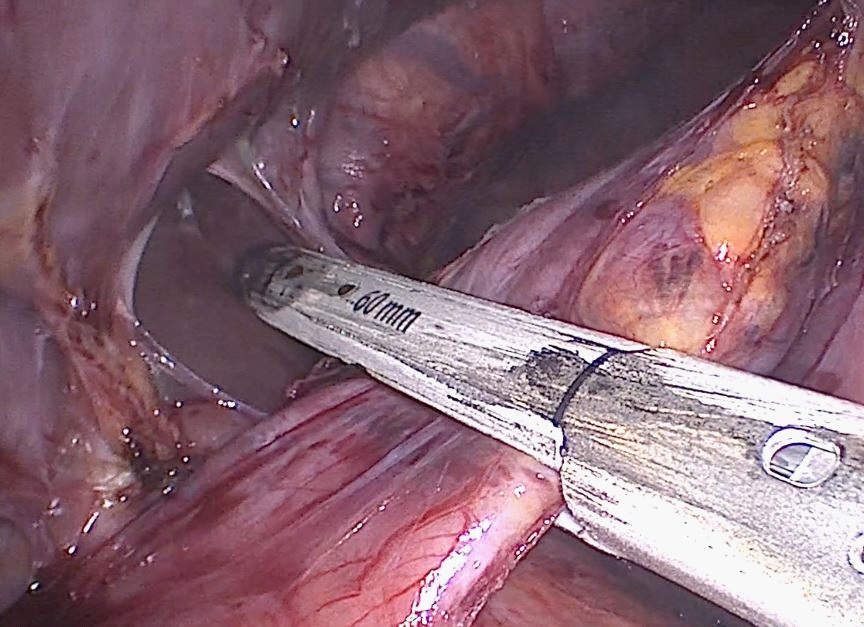
On the current admission, the patient was pale, hypotensive (90/65 mmHg), tachycardiac (110 beats per minute) and tachypneic (25 beats per minute) with 94% SpO2 . Anal exam showed melena. Laboratory findings were unremarkable except for haemoglobin level of 4.6 g/dL. The patient was a nonsmoker and was not on nonsteroidal anti-inflammatory medications. The patient was taken to intensive care unit and resuscitation with 4 U of packed red blood cell was performed, achieving clinical improvement (heart rate 92 bpm, blood pressure 110/65 mmHg, hemoglobin 10.2 g/dL) after which she underwent gastroscopy and computed tomography with the finding of a typical gastric bypass anatomy without a source of bleeding. After day mild hemodynamic symptoms with a decrease in hemoglobin to 9.1 g/dL was found. Resuscitation with another 1 U of packed red blood cell was performed. To determine the localization of gastrointestinal bleeding, technetium-99m red blood cell scintigraphy was performed and revealed bleeding at the gastric fundus (Figure 1). As a result of ongoing hemorrhage, a laparoscopic surgical exploration was undertaken. She was taken to the operating-room and laparoscopic trocars were inserted to the abdomen. In the exploration, the upper abdomen was seen covered with visceral adhesions. After dissection of adhesions, a small anterior gastrotomy was performed on the excluded stomach (Figure 2). The endocamera was inserted from gastrotomy but no blood was observed (Figure 3). Since the bleeding site was determined by scintigraphy, the excluded stomach and the first portion of the duodenum were decided to be resected. After careful dissection, the remnant stomach was released from its adhesions and vascular supply, thus allowing for its resection. With a laparoscopic stapler the first portion of the duodenum was separated above the pancreatic head and ampulla vateri (Figure 4). Resected specimen was taken out of the abdomen from a 10 mm trocar site. The patient was discharged home on postoperative day 3 with a stable hemoglobin level. The histopathological examination of the surgical specimen confirmed a benign nature ulcer at the fundal region of the stomach. At 6 months follow-up, the patient has had no further episodes of gastrointestinal hemorrhage.

Discussion
Marginal ulceration is the most common etiology of upper gastrointestinal bleeding in patients who have undergone gastric bypass surgery therefore it should be considered first in upper gastrointestinal bleeding in patients with gastric bypass. Its reported incidence varies in a wide range between 6% to 12% [6,7]. Fortunately, marginal ulcers can be diagnosed and treated with endoscopy. If there are normal endoscopic findings, the localization of bleeding can be in the remaining excluded stomach and biliopancreatic limb. Bleeding from this area is extremely rare [5,8-10] and diagnostic workup is a very difficult issue because of altered anatomy. Standard endoscopy is limited by its inability to reach the biliopancreatic limb [11]. Even with specialized instruments, it is mostly impossible to reach duodenum and excluded stomach with retrograde endoscopy [12]. In this case, many different methods have been suggested other than peroral endoscopy. These include endoscopy via percutaneous gastrostomy access, computed tomography, angiography, and technetium-99m red blood cell scintigraphy. And also, intraoperative endoscopy of the excluded stomach during exploratory laparotomy can be used [8,13]. If there is not a definitive result from these methods, surgical exploration may be required. Laparoscopic exploration has undeniable advantages over open access in case of stable haemodynamic status, therefore it should be preferred first if possible. An improved understanding of patients’ altered anatomy will ensure physician competence and definitive treatments such as gastric remnant resection can be performed to eliminate the risk of any further complications.
Conclusions
Complications related to gastric remnant should not be forgotten in patients who have undergone mini gastric bypass surgery and present with signs of upper gastrointestinal bleeding. Technetium-99m red blood cell scintigraphy is an effective method to show this kind of bleedings. Surgical (preferably laparoscopic) exploration may be required for diagnose and treatment in such cases.
References
- Tornese S, Aiolfi A, Bonitta G, Rausa E, Guerrazzi G, Bruni PG, et al. Remnant gastric cancer after Roux-en-Y gastric bypass: Narrative review of the literature. Obesity surgery. 2019; 29: 2609- 2613.
- Aleman R, Menzo EL, Szomstein S, Rosenthal RJ. Efficiency and risks of one-anastomosis gastric bypass. Annals of Translational Medicine. 2020; 8.
- Metabolic ASf, Surgery B. Estimate of bariatric surgery numbers. 2011-2017. 2018.
- Grimes KL, Maciel VH, Mata W, Arevalo G, Singh K, Arregui ME. Complications of laparoscopic transgastric ERCP in patients with Roux-en-Y gastric bypass. Surgical endoscopy. 2015; 29: 1753- 1759.
- Patrascu S, Ponz CB, Ananin SF, Soler EMT. A delayed acute complication of bariatric surgery: Gastric remnant haemorrhagic ulcer after Roux-en-Y gastric bypass. Journal of minimal access surgery. 2018; 14: 68.
- Antúnez DJS, Fernández NC, Serrano JO. Unusual case of upper gastrointestinal bleeding after laparoscopic gastric bypass: Erosion of gastric remnant involving a diaphragmatic vessel. Surgery for obesity and related diseases. 2011; 7: 328-329.
- Jordan J, Hocking M, Rout W, Woodward E. Marginal ulcer following gastric bypass for morbid obesity. The American Surgeon. 1991; 57: 286-288.
- Zerey M, Sigmon LB, Kuwada TS, Heniford BT, Sing RF. Bleeding duodenal ulcer after Roux-en-Y gastric bypass surgery. The Journal of the American Osteopathic Association. 2008; 108: 25-27.
- Safatle-Ribeiro AV, Villela EL, de Moura EGH, Sakai P, Mönkemüller K. Hemorrhagic gastritis at the excluded stomach after Rouxen-Y gastric bypass. Endoscopy. 2014; 46: E630-E.
- Sharma A, Houshyar R, Gulati R, Lall C. Massive hemorrhage from unsuspected pseudoaneurysm within an ulcer following” Roux-en-Y” gastric bypass. The American journal of gastroenterology. 2015; 110: 354.
- Peterli R, Borbély Y, Kern B, Gass M, Peters T, Thurnheer M, et al. Early results of the Swiss Multicentre Bypass or Sleeve Study (SM-BOSS): A prospective randomized trial comparing laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass. Annals of surgery. 2013; 258: 690.
- Ivanecz A, Sremec M, Ćeranić D, Potrč S, Skok P. Life threatening bleeding from duodenal ulcer after Roux-en-Y gastric bypass: Case report and review of the literature. World journal of gastrointestinal endoscopy. 2014; 6: 625.
- Braley SC, Nguyen NT, Wolfe BM. Late gastrointestinal hemorrhage after gastric bypass. Obesity surgery. 2002; 12: 404-407.