
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Successful retrieval of a stuck rotablator burr and PTCA balloon by using a guideliner catheter at complex LAD lesion: A case report
Xuan Jin; Moo Hyun Kim*; Kyung Hee Lim; Kai Song
Department of Cardiology, Dong-A University Hospital, Busan, Republic of Korea.
*Corresponding Author : Moo Hyun Kim
Department of Cardiology, Dong-A University Hospital, 26 Daesingongwon-ro, Seo-gu, Busan 49201,
Republic of Korea.
Email: kimmh@dau.ac.kr
Received : Apr 01, 2021
Accepted : Apr 28, 2021
Published : Apr 30, 2021
Archived : www.jcimcr.org
Copyright : © Kim MH (2021).
Abstract
Background: An entrapped rotablator burr is a rare but severe complication of Rotational Atherectomy (RA), and surgical removal is invasive and takes several hours. Therefore, a less invasive measure is necessary for this complication.
Case summary: A 54-year-old man with Diabetes Mellitus (DM) and hypertension revealed chronic total occlusion in the proximal LAD In-Stent Restenosis (ISR). The left coronary ostium was engaged with 7Fr EBU. A Runthrough was inserted into D1, and the XTR guidewire was inserted into distal LAD using Guideliner catheter. Because of the severe angulated calcified lesion at the proximal LAD, the 1.0 balloon could not pass the lesion, so we performed rotablation. The burr suddenly became trapped within the calcified lesion at the distal angulated edge. We performed a gentle manual retraction of the rota and attempted to insert another guidewire to alongside the burr for balloon dilation to free the burr, but wiring failed. Then, we cut off the drive sheath of the rota, inserted a 5.5 Fr Guideliner catheter through the remaining system and fixed the catheter tip near the entrapped rotablator burr by pushing and pulling the rotablator at the same time. Finally the rota system was removed successfully, but the burr was nearly detached from the rota wire during retraction.
Discussion: We might get an information of the degree of fibrous and angulated calcification by MDCT before PCI and this will be helpful to predict the possibility of bur stuck. A large size sheath and femoral approach may be preferable.
Keywords: Coronary artery disease; Chronic total occlusion; Rotational atherectomy; Burr entrapment; Guideliner.
Citation: Jin X, Kim MH, Lim KH, Song K. Successful retrieval of a stuck rotablator burr and PTCA balloon by using a guideliner catheter at complex LAD lesion: A case report. J Clin Images Med Case Rep. 2021; 2(2): 1097.
Introduction
The rotablator was a suitable and irreplaceable device used to remove heavily calcified lesions in current Percutaneous Coronary Intervention (PCI). An entrapped rotablator burr was a rare but life-threatening complication due to the difficulty in retrieval [1]. There were several bailout endovascular approaches that have been proposed, including gentle manual traction, passing of another guide wire followed by balloon inflation to release the trap, using a snare proximal to the burr for forceful local traction, or a child-in-mother catheter to facilitate the successful retrieval [2]. We presented a case of successful rescue of stuck rotablator burr entrapment using a Guideliner catheter.
Timeline
20 years prior |
PCI for pRCA, mLAD and dLAD |
2001.12.08 |
m-LADà S670 3.0 x 15mm |
2002.02.15 |
m-LAD re PCI with cut 3.25mm balloon |
2002.02.20 |
OMà Directional coronary atherectomy 3.0-3.4 |
2006.10.10 |
m-LAD à re PTCA |
2 months prior |
MDCT showed diffuse dense calcification and luminal narrowing at pLAD (previous inserted stent), markedly decreased ejection fraction of left ventricle with dilatation |
Re-admission to the hospital |
The patient presented with chest pain. Echocardiogram showed LVEF was 30-34% and suggested ischeamic heart disease with moderate to severe LV dysfunction, moderate LVE, mild LAE with elevate LV filling pressure. |
Day 2 |
Percutaneous coronary intervention was performed. |
Day 4 |
The patient was discharged after SPECT. SPECT showed severe myocardial infarction in LAD territory and severe LV systolic dysfunction with global hypokinesia. |
Visit 1 |
The patient’s symptoms remained as before and considered CABG if necessary. |
Case presentation
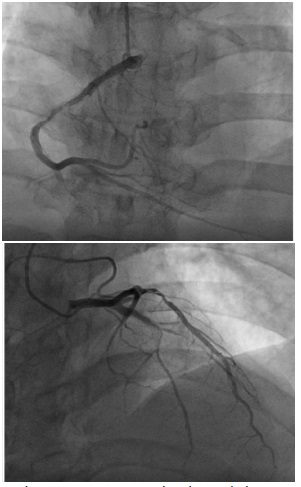
A 54-year-old man was admitted to our hospital with unstable angina. The patient’s coronary risk factors were Diabetes Mellitus (DM) and hypertension, and had past medical history of previous Myocardial Infarction (MI), Chronic Heart Failure (CHF) and Cerebrovascular Accident (CVA). Initial coronary angiography showed chronic total occlusion in the proximal Left Anterior Descending artery (LAD) In-Stent Restenosis (ISR), as well as diffusely calcified stenosis in mid Right Coronary Artery (RCA) and distal Left Circumflex Artery (LCx) (Figure 1).
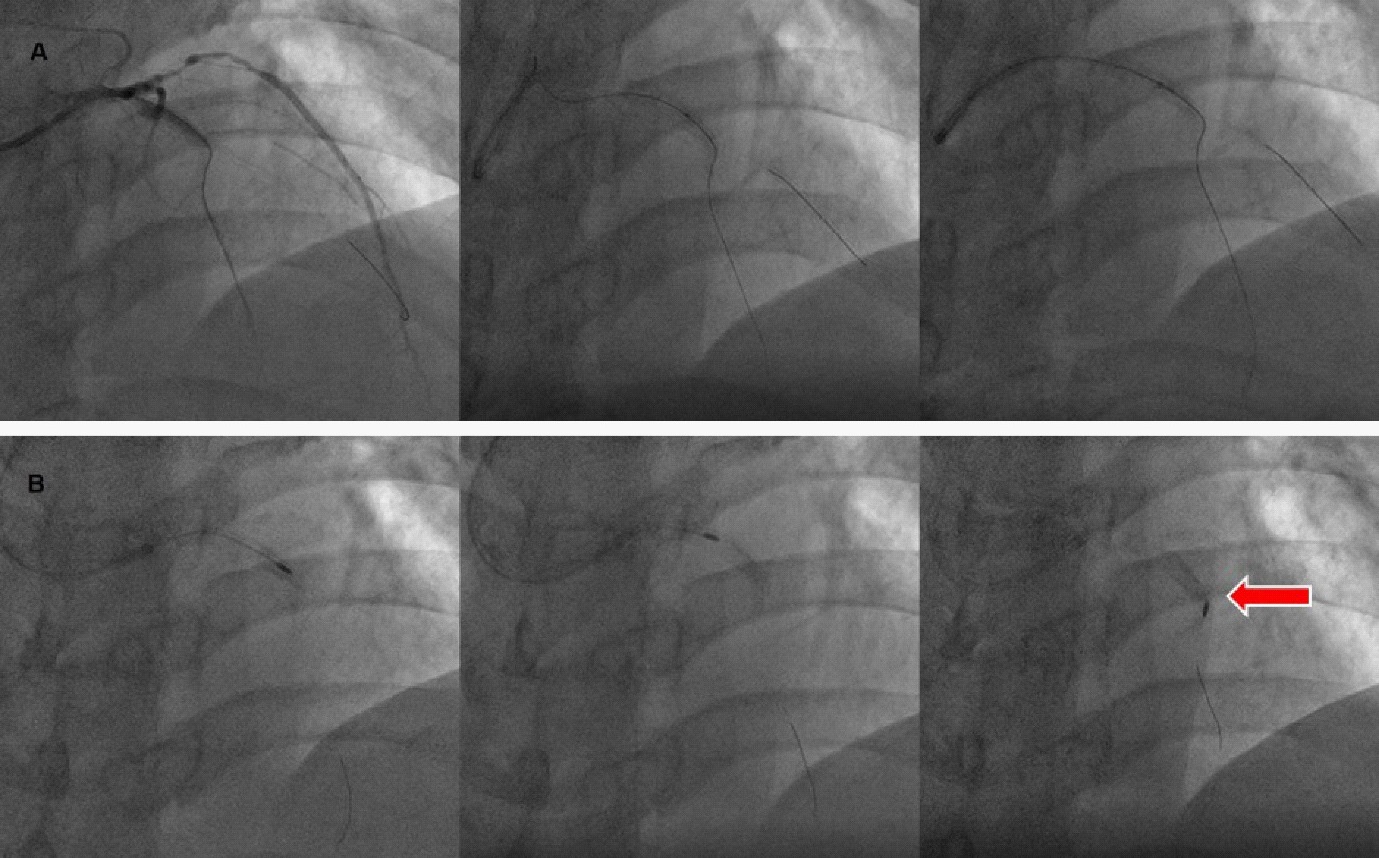
A 6 Fr sheath was inserted into the right brachial artery, and the left coronary ostium was engaged with 6 Fr EBU 3.5 guiding catheter. A Runthrough guidewire was inserted into D1, and the Sion guidewire couldn’t cross the proximal LAD lesion, so the guidewire was changed to XTR with Guideliner catheter, then inserted into distal LAD successfully (Figure 2A). Because of the severe angulated calcified lesion at the proximal LAD in-stent restenosis, the 1.0 X 6 mm IKAZUCHI Zero balloon could not pass the lesion, so we decided to perform rotablation.
The sheath was changed to 7 Fr and guiding catheter was changed to 7 Fr EBU 4.0 guiding catheter. A Finecross microcatheter was used to exchange the wire for the rota guidewire. Rotablation was performed using a 1.25 mm burr initially, short runs of 10 sec were performed at 200,000 rpm, and multiple sessions of ablation were unsuccessful in crossing the lesion. The burr suddenly stalled and became trapped within the heavily calcified lesion at the distal portion of the proximal stent (Figure 2B). At that time, the patient produced heart block with bradycardia and atropine was given intravenously.
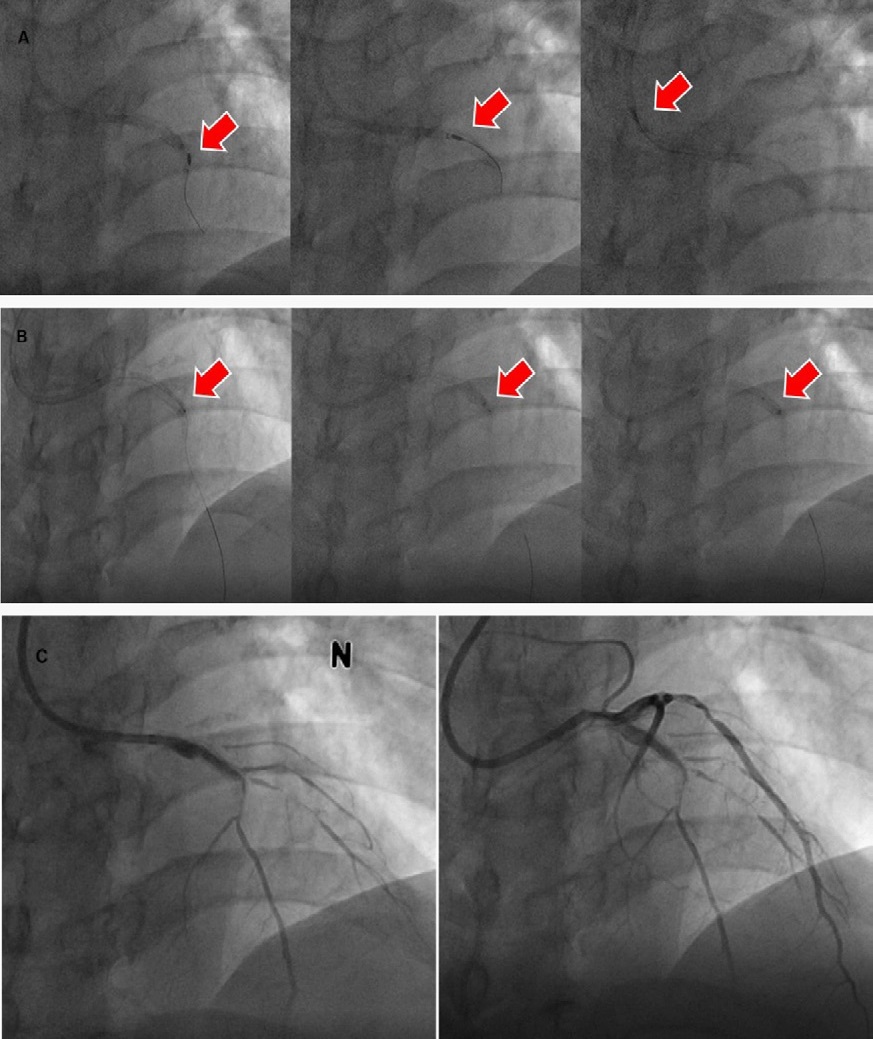
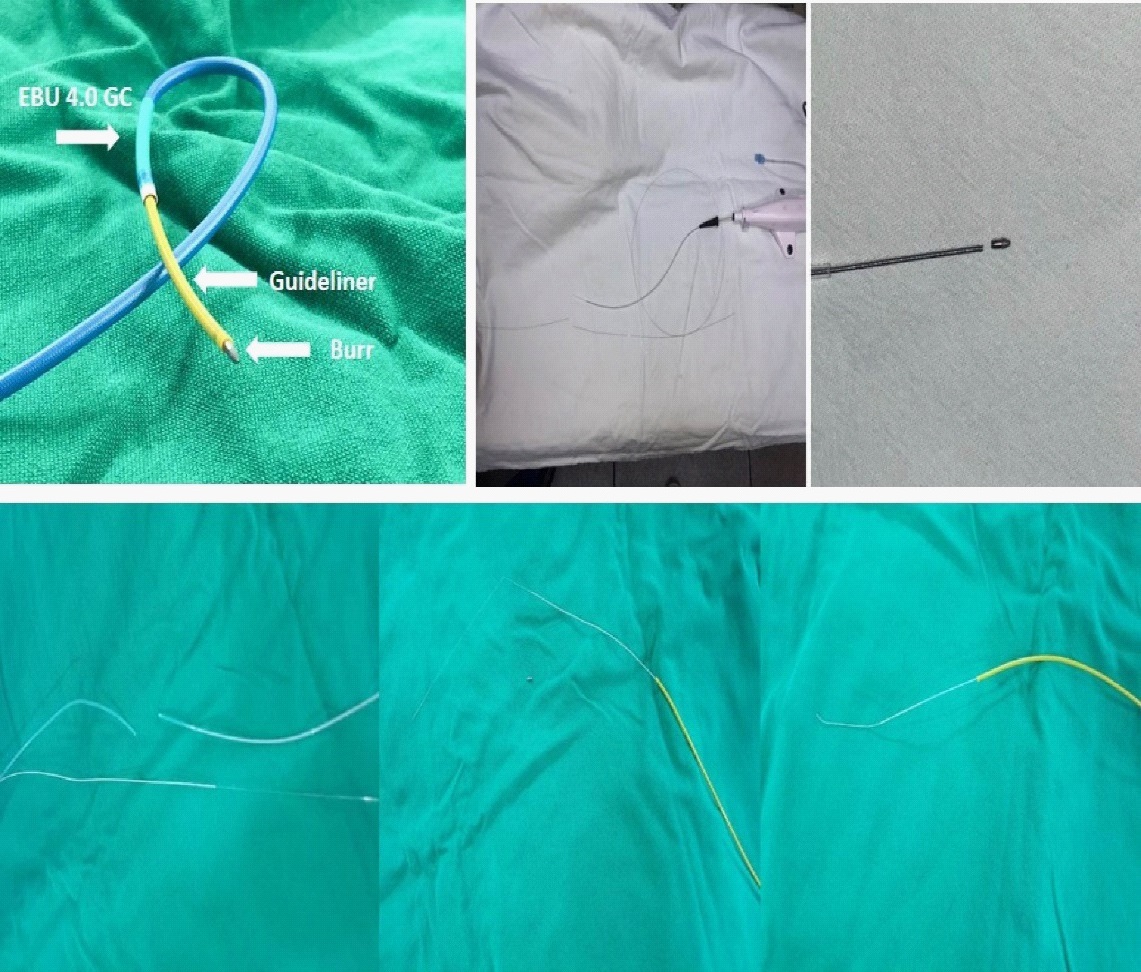
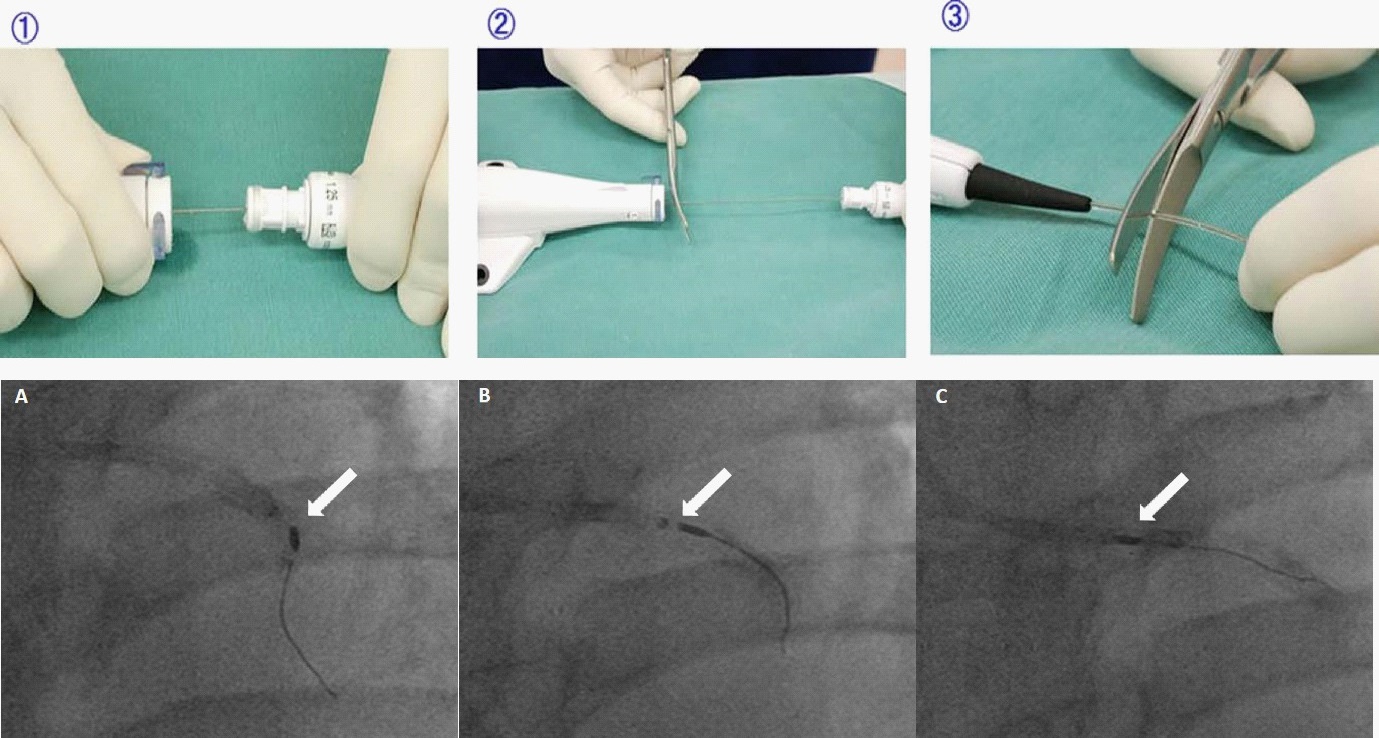
Firstly, we attempted to a gentle manual pull back of the rotablator system, but was unsuccessful. Extreme force may damage on the vessel or the burr and burr shaft, resulting in shaft fracture. Secondly, we attempted to insert a Run through guidewire to alongside the burr for balloon dilation to free the burr, but wiring failed. Then, we cut off the drive sheath and the sheath of the rotablator, inserted a 5.5 Fr Guideliner catheter through the remaining rotablator system and fixed the catheter tip near the entrapped rotablator burr by pushing and pulling the rotablator at the same time (Figure 3A). Finally the rota system was removed successfully (Figure 5), but the burr was nearly detached from the rota wire during retraction, the best out of the worst, it happened inside the Guideliner (Figure 4). PCI continued after the patient stabilized after some treatment, we attempted to dilate the 1.0 X 6 mm balloon with 6 atm several times, but the balloon still cannot pass the lesion and balloon stuck again within the severe calcified lesion (at the same site of rota stuck). So we had to use the Guideliner catheter agian and pull back the balloon successfully (Figure 4). The angiogram showed similar imaging as prior to the intervention (Figure 3C). In consideration of the unstable state of patient, we recommended CABG.
Discussion
In severe angulated and calcified lesion, a 7-8Fr sheath through the femoral approach may be preferable. Before PCI, we could predict the degree of fibrotic calcification and angulated lesion with MDCT.
PCI has been increasingly performed for complex calcified lesions with an incremental need for Rotational Atherectomy (RA) to facilitate balloon / stent delivery and adequate device expansion. Most complications of RA are common to all PCI procedures, such as peri-procedural myocardial infarction, vascular access complications, coronary dissection, abrupt vessel closure and perforation. However, there are complications solely due to the RA procedure such as slow flow / no reflow, bradycardia and atrioventricular block, or specific to the rotablator system such as burr entrapment and rota wire fracture [3]. Burr entrapment is a rare but serious complication of RA, and the risk of these complications is greater in angulated calcified lesion [4,5]. Although surgical removal with coronary bypass graft is the most reliable method, the primary therapeutic option remains interventional retrieval by means of the step-by-step approach. Most operators realize that there is greater risk of complications when using rotational atherectomy in an angulated calcified lesion, however, we had no other alternative but to perform rotational atherectomy if balloon dilatation does not work for these tough lesions [4,6].
The step-by-step algorithm for the measurement of an entrapped rotablator burr as follows: (1) Re-cross with a second wire; (2) Removal with a snare; (3) Removal with a child-inmother catheter; (4) Surgical removal [7]. Most of the previous cases used the child-in-mother catheter to remove the stuck rotablator, and a 120 cm straight guiding catheter was recommended, and Heartrail ST01 was most frequently used [8]. In this case, we tried to use balloon dilation to free the burr, but the guidewire could not insert to alongside the burr. So we used a 5.5 Fr Guideliner catheter to retrieve the entrapped rotablator burr. The Guideliner catheter was a coaxial guiding extension just like ST01, and its monorail structure provides easier delivery of other devices. Although we succeeded in retrieving the burr by pushing the Guideliner catheter as well as simultaneously pulling the rotablator system, but the terrible situation was that the burr and rota wire were nearly broken during retraction. Fortunately this happened in the catheter and burr did not remain in the vessel. This may be due to severe calcification in stent restenosis and angular calcification. For the severe angulated calcified lesion, Sakakura et.al. [9] expanded the lesion modification hypothesis: To make a crack using a small rotational atherectomy only on the straight part of the continuous calcification. We can try balloon dilatation (noncompliant balloon) beyond the angle. The balloon dilatation would likely cause a continuous crack beyond the angle because the edge of the crack would receive high pressure produced by balloon dilation.
Conclusions
In conclusions, rotational atherectomy burr stuck at an angulated calcified lesion is challenging situation and this could be retrieved by using Guideliner catheter after cutting the rotasystem.
Statement of consent: The authors confirm that written consent for submission and publication of this case report including images and associated text has been obtained from the patient in line with COPE guidance.
References
- Grise MA, Yeager MJ, Teirstein PS. A case of an entrapped rotational atherectomy burr. Catheter Cardiovasc Interv. 2002; 57: 31–33.
- Chiang CH, Liu SC. Successful retrieval of an entrapped rotablator burr by using a Guideliner guiding catheter and a snare. Acta Cardiologica Sinica. 2017, 33 (1): 96.
- Lindsay A, Chitkara K, Di Mario C. Complications of Percutaneous Coronary Intervention. Springer, London. https://doi. org/10.1007/978-1-4471-4959-0_29.
- Yamamoto S, Sakakura K, Funayama H, Wada H, Fujita H, Momomura S-i. Percutaneous Coronary Artery Bypass for Type 3 Coronary Perforation. JACC: Cardiovascular Interventions. 2015; 8: 1396-1398.
- Sakakura K, Ako J, Momomura S-i. Successful removal of an entrapped rotablation burr by extracting drive shaft sheath followed by balloon dilatation. Catheter Cardiovasc Interv. 2011; 78: 567-570.
- Pedersen WR, Goldenberg IF, Johnson RK, Mooney MR. Successful rotational atherectomy in the setting of extensive coronary dissection: A case of failed balloon angioplasty in a nondilatable calcified lesion complicated by balloon rupture and extensive dissection. Catheter Cardiovasc Interv. 2003; 59: 329-332.
- Sulimov DS, Abdel-Wahab M, Toelg R, Kassner G, Geist V, Richardt G. Stuck rotablator: The nightmare of rotational atherectomy. EuroIntervention. 2013; 9: 251-258.
- Kimura M, Shiraishi J, Kohno Y. Successful retrieval of an entrapped Rotablator burr using 5 Fr guiding catheter. Catheter Cardiovasc Interv. 2011; 78: 558-564.
- Sakakura K, Taniguchi Y, Matsumoto M, Wada H, Momomura S, Fujita H. How Should We Perform Rotational Atherectomy to an Angulated Calcified Lesion?. Int Heart J 2016; 57: 376-379.