
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A sign of spinal cord stroke. Vertebral body ischemia
Raquel Mitjana1; Gerard Mauri-Capdevilla2; Francisco Purroy2; Daniel Vázquez-Justes2; Mikel Vicente-Pascual2*
1 Image Diagnostic Institute, Section of Neuroradiology, Arnau de Vilanova University Hospital, University of Lleida, Lleida, Spain.
2 Stroke Unit, Department of Neurology, Arnau de Vilanova University Hospital, University of Lleida, Lleida. Spain.
*Corresponding Author : Mikel Vicente-Pascual
Stroke Unit, Neurology Department, Arnau de
Vilanova University Hospital, Av. Alcalde Rovira
Roure, 80, 25198 Lleida, Spain.
Email: mvpascual.1@gmail.com
Received : Apr 01, 2021
Accepted : Apr 29, 2021
Published : May 04, 2021
Archived : www.jcimcr.org
Copyright : © Vicente-Pascual M (2021).
Abstract
Spine cord infarction is a rare neurological disease. The MRI can show T2 hyperintense signals, and these lesions can be associated with a vertebral body lesion, that supports the ischemic etiology.
We present a 54 year-old-woman with an acute spinal cord syndrome, with a final diagnosis of spinal cord infarction. The initial MRI showed no abnormalities, but a second MRI showed increased signal intensity in T2 sequences and DWI, with a decreased in ADC maps, all compatible with an ischemic lesion. Moreover, the MRI revealed a T2 hyperintense signal in adjacent vertebral body, compatible with ischemic nature.
Spine cord MRI is an important complementary exploration in the diagnostic of myelitis syndrome. Other sequences, such as diffusion, should be included, as well as consider the coexistence of a lesion in the adjacent vertebral body, which can support the ischemic etiology of the symptoms.
Keywords: Stroke, Infarction, Spinal cord, Vertebral body, MRI
Citation: Mitjana R, Mauri-Capdevilla G, Purroy F, Vázquez-Justes D, Vicente-Pascual M. A sign of spinal cord stroke. Vertebral body ischemia. J Clin Images Med Case Rep. 2021; 2(3): 1099.
Introduction
Acute spinal cord syndrome is a diagnostic challenge for the neurologist. The cause is not found over 50% of cases, although an exhaustive study is realized [1]. The spinal cord infarction is one of its etiologies. It is a rare disease, representing only 1.2% of all vascular neurological diseases [2]. Between complementary examinations, spinal MRI may show T2 hyperintense signal and a restriction in diffusion sequences, but the image can show no abnormalities. The ischemia in the vertebral body is a radiological data that supports the ischemic nature, although not always is visible.
Case report
We present a 54 year-old-woman, with history of unknown collagen disease, who suffered sudden back and legs pain, followed by weakness of both legs. On admission she had a 3/5 paraparesis. The weakness progressed in 6 hour to a total paresis.
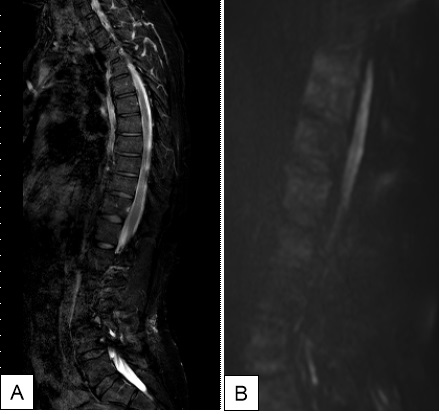
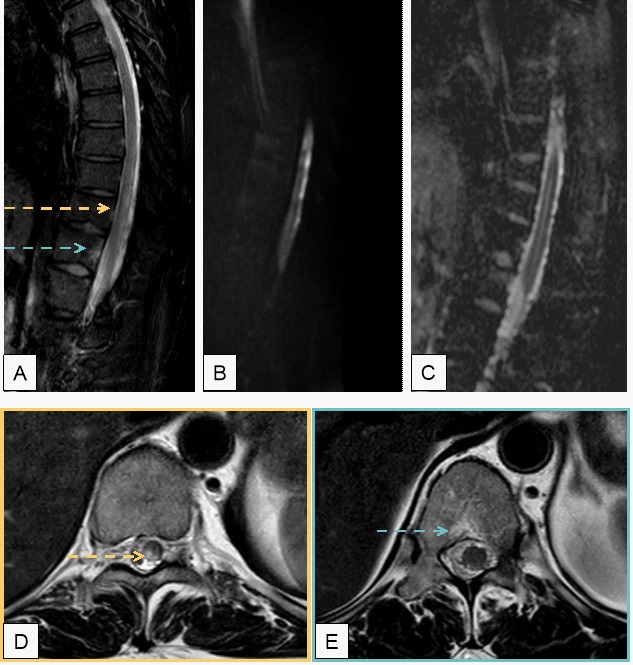
An MRI performed on the admission day showed no abnormalities (Figure 1). Blood and cerebrospinal fluid analysis, (including serologies and auto-immunity) had no significant results. A follow-up MRI performed seven days later showed T2 hyperintense signals in the dorsal T8 to T11 spinal cord and vertebral body (Figure 2), with increased signal intensity on Diffusion-Weighted Imaging (DWI) and reduced in Apparent Diffusion Coefficients (ADC) maps. A thoraco-abdominal angioCT and spinal arteriography did not show vascular alterations, and an echocardiogram and monitoring for more than 72 hours ruled out embolism alterations. With the diagnosis of spinal cord stroke she received anti-platelet and lower lipid treatment and she started rehabilitation.
Discussion
The spinal cord syndrome is a rare condition. It is presented with a paraparesis and a sensitive alteration in legs or an inferior part of the body. Between its etiologies the cord infarction represents a rare cause [2]. The spinal MRI is important to confirm the diagnosis, showing T2 hyperintense signal, which is not specific of infarct lesions [1], because neoplasms, infections, multiple sclerosis or other inflammatory lesions may also show this image. Previous reports described abnormal MRI-T2 signals in the vertebral body that coexist with spinal cord infarction and can support ischemic nature [3-8]. However, bone marrow alterations can be seen in other pathologies such as fractures, infections, tumours and degenerative pathologies. Typically, acute ischemia is presented with increased signal intensity on DWI with corresponding decreased diffusivity on the calculated ADC maps. Despite these, there are few cases reported that show hyperintensity in DWI in acute spinal artery infarction [9,10]. Our case report shows these two changes. The MRI shows a hyperintense spinal cord lesion in T2 sequences, which is accompanied by T2 hyperintense signal in vertebral body. Besides that, there is an increased signal in DWI with corresponding reduction in ADC maps that reveals the ischemic etiology.
Conclusion
We present a characteristic image that was essential to get to the diagnosis of ischemic myelitis. The etiology of an acute spinal cord syndrome is extensive, and treatment and prognosis depend on it. Spine cord MRI should include specific sequences such as diffusion, as well as consider the coexistence of a lesion in the adjacent vertebral body and its characteristics so it can support the ischemic etiology.
References
- Martinelli V, Comi G, Rovaris M, Filippi M, Colombo B, Locatelli T, Campi A, Rodegher M, Canal N. Acute myelopathy of unknown aeti- ology: A clinical, neurophysiological and MRI study of shortand long-term prognostic factors. J Neurol. 1995; 242: 497–503.
- Sandson TA, Friedman JH. Spinal cord infarction: Report of 8 cases and review of the literature. Medicine (Baltimore). 1989; 68: 282–292 .
- Faig J, Busse O, Salbeck R. Vertebral body infarction as a confirmatory sign of spinal cord ischemic stroke: Report of three cases and review of the literature. Stroke. 1998; 29: 239-243.
- Suzuki T, Kawaguchi S, Takebayashi T, Yokogushi K, Takada J, Yamashita T. Vertebral body ischemia in the posterior spinal artery syndrome: Case report and review of the literature. Spine (Phila Pa 1976). 2003; 28: E260-E264.
- Mikulis DJ et al. Spinal cord infarction and ®brocarti- lagenous emboli. AJNR Am J Neuroradiol. 1992; 13: 155-160.
- Yuh WTC et al. MR imaging of spinal cord and vertebral body infarction. AJNR Am J Neuroradiol. 1992; 13: 145-154.
- Haddad MC, Aabed Al-Thaga® MY, Djurberg H. MRI of spinal cord and vertebral body infarction in the anterior spinal artery syndrome. Neuroradiology 1996; 38: 161-162.
- Börnke C, Schmid G, Szymanski S, Schöls L. Vertebral body infarction indicating midthoracic spinal stroke. Spinal Cord. 2002; 40: 244-247.
- Bammer R, et al. Diffusion-weighted MR imaging of the spinal cord. AJNR Am J Neuroradiol. 2000; 21: 587-591.
- Muscat P, et al. Vertebral artery dissection in Turner's syndrome: diagnosis by magnetic resonance imaging. J Neuroimaging. 2001; 11: 50-54.