
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Suture thread: An unusual etiology of tracheal pseudotumor
Adelaide Alves*; Sofia Neves; José Almeida
Pulmonology Service of the Hospital Center of Vila Nova de Gaia / Espinho, Vila Nova de Gaia, Portugal.
*Corresponding Author : Adelaide Alves
Pulmonology Service of the Hospital Center of Vila
Nova de Gaia / Espinho, Vila Nova de Gaia, Portugal.
Email: adelaide.pereira.alves@gmail.com
Received : Apr 02, 2021
Accepted : Apr 29, 2021
Published : May 04, 2021
Archived : www.jcimcr.org
Copyright : © Alves A (2021).
Citation: Alves A, Neves S, Almeida J. Suture thread: An unusual etiology of tracheal pseudotumor. J Clin Images Med Case Rep. 2021; 2(3): 1106.
Description
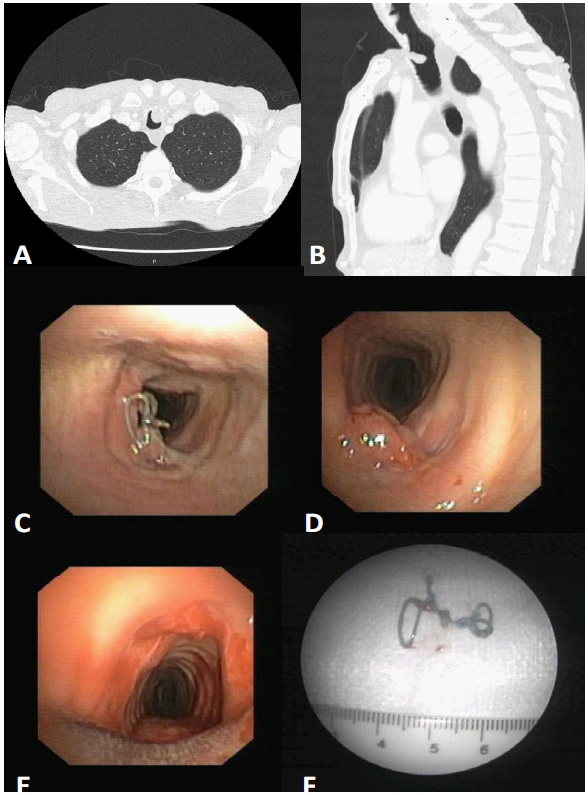
A 66-year-old man ingested sodium hydroxide in a suicide attempt in June 2018. In emergency room, he presented burning of the tongue and uvula and supraglottic and vocal cords edema. Because of the risk of airway obstruction, the patient underwent endotracheal intubation and started invasive mechanical ventilation. Five days later, a surgical tracheostomy was performed due to a large laryngeal necrosis including extensive epligottis involvement. After prolonged mechanical ventilation through tracheostomy, the patient presented a favorable clinical course allowing ventilator weaning and decannulation 2 months after initial presentation. In February 2019, cervical Computed Tomography (CT) revealed a polypoid lesion occupying 25% of the tracheal lumen, with contrast uptake and suggestive of malignant etiology (Figure 1A-B). The patient was asymptomatic. Rigid bronchoscopy showed that the pseudotumoral tracheal lesion corresponded to granulation tissue around suture thread from the previous tracheostomy, which were successfully removed during the procedure (Figure 1C-E). Pathological examination showed granulation tissue with extensive inflammatory infiltrate and foreign-body giant cell reaction.
The formation of granulation tissue and tracheal stenosis are recognized late complications of tracheostomy. Endo-tracheal foreign bodies may increase the risk of these complications mimicking malignant lesions. Bronchoscopy plays a key role in the diagnosis and treatment of these complications [1,2].
References
- Epstein SK. Late complications of tracheostomy. Respir. Care. 2005; 50: 542-549.
- Sarper A, Ayten A, Eser I, et al. Tracheal stenosis after tracheostomy or intubation. Review with special regard to cause and management. Tex Heart Inst J. 2005; 32: 154-158.