
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Fulminant case of multiple sclerosis (marburg variant) with atypical MRI presentation
Luca Mancinelli1; Yerma Bartolini1; Maria Lia Cataldi2; Chiara Bomprezzi1; Alessia Tomassini3; Manila Antonelli4; Francesca Gianno4,5; Daniela Bartolini6; Maria Ruggiero2; Marco Longoni1*
1 Neurology Unit, Maurizio Bufalini Hospital, Viale Ghirotti 286–47521 Cesena, Italy
2 Neuroradiology Unit, Maurizio Bufalini Hospital, Viale Ghirotti 286–47521 Cesena, Italy.
3 Neurosurgery Unit, Maurizio Bufalini Hospital, Viale Ghirotti 286–47521 Cesena, Italy.
4 Department of Radiological, Oncological and Pathological Sciences, Sapienza University of Rome, Piazzale Aldo Moro 5 - 00185 Rome, Italy.
5 IRCCS Neurological Institute of Southern Italy NEUROMED, Neuropathology Research Unit, Ospedale IRCCS Neuromed, Via Atinense 18 - 86077 Pozzilli (IS), Italy
6 Anatomic Pathology Unit, Maurizio Bufalini Hospital, Viale Ghirotti 286–47521 Cesena, Italy
*Corresponding Author : Marco Longoni
Neurology Unit, Maurizio Bufalini Hospital, Viale Ghirotti 286–47521 Cesena, Italy.
Email: marco.longoni@auslromagna.it
Received : Apr 03, 2021
Accepted : Apr 30, 2021
Published : May 05, 2021
Archived : www.jcimcr.org
Copyright : © Longoni M (2021).
Abstract
Marburg type is a rare variant of Multiple Sclerosis (MS) characterized by a severe and progressive course/evolution leading to exitus in few months. Its radiological presentation commonly raises suspicion of a malignancy, often requiring a brain biopsy for histological confirmation.
Hereby we report an atypical radiological presentation and progression of a pathologically confirmed case of Marburg MS
Keywords: Multiple Sclerosis; Marburg variant; Magnetic resonance imaging.
Citation: Longoni M, Mancinelli L, Bartolini Y, Cataldi ML, Bomprezzi C. Fulminant case of multiple sclerosis (marburg variant) with atypical MRI presentation. J Clin Images Med Case Rep. 2021; 2(3): 1108.
Introduction
Firstly described in 1906, Marburg type Multiple Sclerosis (MS) is a rare acute demyelinating disease characterized by a fulminant course of few months, often presenting with hemiplegia, hemianopia, aphasia, seizures and confusion and affecting mainly young adults. Histopathological findings typically show large tumor-like demyelinating plaques in the centrum ovale and hypercellular demyelinating plaques, with oedema, faint astroglial reaction, and giant astrocytes [1].
On MRI scans, the typical presentation consists of pseudotumoral demyelinating lesions, which have been classified according to MAGNIMS consensus in four main types: Ring- like, megacystic, infiltrative and Balò-like [2]. Here we report a case of Marburg type MS with an atypical radiological presentation.
Case report
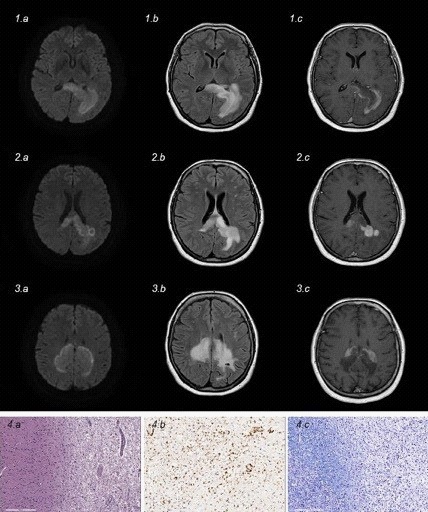
A 53-years-old woman with unremarkable past medical history presented at our emergency department in June 2019 complaining of progressive confusion, memory impairment and right hemianopia. An unenhanced head CT scan showed a left parieto- occipital hypodensity with mass effect requiring urgent neurosurgery review and admission. The gadolinum-enhanced brain MRI scan confirmed the presence of a large irregular and predominantly rim-enhanced lesion involving the left forceps major and extended to the adjacent peritrigonal white matter, lateral ventricular ependymal lining and splenium of the corpus callosum (Figures 1a,b,c). Brain MRI spectroscopy showed an inverted NAA-Cho and NAA-Cr ratios with presence of lipids and lactate.
Spinal cord MRI scan was normal and CSF analysis showed mild increase in protein and a pattern 3 at serum-CSF Isoelectro-Focusing (IEF) (see Table 1). Brain lymphoma was firstly hypothesized and the patient underwent brain biopsy revealing only histiocytic- macrophagic infiltrate supportive of a diagnosis of inflammatory-demyelinating lesion.
Table 1: Laboratory findings.
Exam |
Notable results |
Notes |
CSF: physical-chemical and indices |
Proteins 0.66 g/l (0.20-0.40); Total cell count 4/microliter; |
First lumbar puncture (2019 Jun 26th) |
CSF-serum IEF |
Pattern 3 oligoclonal bands |
First lumbar puncture |
CSF: culture |
Negative for bacteria and yeast |
First lumbar puncture (2019 Jun 26th) |
CSF: physical-chemical |
Proteins 0.72 g/l (0.20-0.40); Total cell count 2/microliter; |
Second lumbar puncture (2019 Oct 3rd) |
CSF-serum IEF |
Pattern 4 oligoclonal bands |
Second lumbar puncture |
Serum cryoglobulins |
Absent |
|
Lupus anticoagulant |
Negative |
|
Serology for HIV, HBV, HCV, Borrelia, Treponema |
Negative |
|
CSF: polymerase chain reaction for JCV, VZV, EBV, CMV, Toxoplasma |
Negative |
Second lumbar puncture |
Quantiferon TB Gold |
Negative |
|
ANA, MPO-ANCA, PR3-ANCA, ENA, anti |
Negative |
|
Serum anti-neuronal Ab (amphiphysin, CV2.1, Ma-2/TA, Ri, Yo, Hu) |
Negative |
|
Regardless high dose pulse intravenous steroids therapy (methylprednisolone 1000 mg daily for five days) started few weeks after biopsy, her condition progressed with increasing confusion and right arm apraxia.
A new MRI scan performed three weeks after steroid therapy showed radiological progression with symmetrical growth in every directions, significant rim enhancement and peripheral patchy diffusion restriction particularly at the leading edge (Figures 2 a,b,c).
She was then admitted to the Neurological department and a repeat lumbar puncture showed only mild CSF protein elevation and an IEF pattern 4. A complete laboratory workup, including screening for systemic autoimmune diseases as well as infectious agents, did not suggest other conditions (Table 1). Total body CT scan and Positron Emission Tomography (PET) did not reveal pathological conditions. CSF and serum analysis resulted negative for Anti-Myelin Oligodendrocyte Glycoprotein (MOG) antibodies.
She was treated with Intravenous Immunoglobulin (IVIG) 2 gr/kg divided in 5 administrations, again with no effect, rather with persistent deterioration consisting in a progressive right hemiparesis with contralateral lower limb paresis, painful diffuse dysesthesia and worsening of previous symptoms.
The patient and her relatives denied any further therapies and decided for voluntary discharge. Nevertheless, after few weeks she was re-admitted in our department because of progressive worsening. Neurological examination demonstrated a further decline in clinical conditions leading to mutacism, tetraparesis, diffuse pain with hyperalgesia and anorexia.
She was treated with Rituximab 1000 mg iv without clinical improvement and MRI performed two weeks later evidenced a further enlargement of the lesion with persistent peripheral enhancement and diffusion restriction at the leading edge (Figures 3 a,b,c). Considering the progressive clinical course despite immunosuppressive therapies, decision for palliative care was made in agreement with her relatives, until she died few days later.
A brain autopsy study revealed areas of demyelination with diffuse infiltrate of CD68+ foamy histiocytes in the white matter, together with lymphocytes and plasmacells with a perivascular distribution and with relatively preserved axons. A reactive gliosis with gemistocytic elements expressing the Glial Fibrillary Acidic Protein (GFAP) was also evident. Combined with previous biopsy features, these findings supported the diagnosis of an acute, progressive and fulminant demyelinating disease like Marburg variant of MS (Figures 4 a,b,c).
Discussion
In this case we describe an atypical MRI pattern and progression of a Marburg variant of MS. Indeed, the leading edge of the lesion, which looks like a front line of fire leaving behind scorch earth, could suggest Progressive Multifocal Leukoencephalopaty (PML) instead of an acute inflammatory demyelinating process (Figures). Nevertheless, brain tumor was also considered because of gadolinium enhancement, whereas gray matter sparing suggested a possible diagnosis of leukodystrophy. However, CSF and brain autopsy were negative for JCV DNA and malignancies and the rapid clinical course ruled out inherited white matter diseases.
Further, before the diagnostic confirmation was achieved by brain autopsy, the complete absence of clinical effectiveness of immunotherapies and sharp disease progression keep feeding the uncertainty of the diagnosis despite brain biopsy result. Indeed, as it was previously described by Gupta et al. in patients with cerebral neoplasms, if the sample is collected at the periphery of the lesion a false diagnosis of demyelinating process can be supported [3].
Our patient had no clinical benefit from steroids, IVIG and rituximab. The latter was chosen, rather than approved MS disease modifying therapies, considering that the differential diagnosis of lymphoma was never definitely excluded by the neuroradiological findings and clinical course. Moreover, some cases of primary CNS lymphoma with finds of non-specific inflammation or demyelination with axonal sparing at initial biopsy have been documented [4]. Finally, rituximab has been effectively used in antibody mediated conditions like Neuromyelitis Optica Spectrum Disorder (NMOSD) and anti-MOG syndromes, which were also included in the differential diagnoses.
We believe that the really atypical feature of this fulminant MS case lies in its MRI appearance and evolution. Indeed, the lesion exhibited a classic infiltrative growth pattern, characteristic of malignancies, and a peripheral Gd enhancement with patchy diffusion restriction particularly at the leading edge, evoking PML. Even though infiltrative is one of the four possible MRI pattern of pseudotumoral demyelinating lesions, in fulminant MS - Marburg variant - Capello has described that follow-up MRI usually reveals the shrinkage of the lesion after treatment with steroids or, on the contrary, the appearance of new areas of demyelination [1]. Our patient did not present none of either.
With this case report we finally aim to bring to the attention of clinicians this highly atypical radiological presentation and progression of Marburg MS, which necessitated post-mortem pathological examination for final diagnosis.
Conflict of interest
Dr. Mancinelli reports personal fees from Merck Serono, Biogen, Sanofi Genzyme, Novartis; grants from Teva and Roche, outside the submitted work. Dr. Y. Bartolini has nothing to disclose. Dr. Cataldi has nothing to disclose. Dr. Bomprezzi has nothing to disclose. Dr. Tomassini has nothing to disclose. Dr. Antonelli has nothing to disclose. Dr. Gianno has nothing to disclose. Dr. D. Bartolini has nothing to disclose. Dr. Ruggiero has nothing to disclose. Dr. Longoni has nothing to disclose.
References
- Capello E, Mancardi GL. Marburg type and Balò’s concentric sclerosis: Rare and acute variants of multiple sclerosis. Neurol Sci. 2004; 25: S361-363.
- Seewann A, Enzinger C, Filippi M, Barkhof F, Rovira A. et al. MRI characteristics of atypical idiopathic inflammatory demyelinating lesions of the brain: A review of reported findings. J Neurol. 2008; 255: 1-10.
- Gupta K, Mehta S, Ahuja CK, Salunke P, Sharma N. Glioblastoma multiforme masquerading as a tumefactive demyelinating lesion: Lessons learned at autopsy. Neurol India. 2016; 64: 737- 741.
- Alderson L, Fetel MR, Sisti M, Hochberg F, Cohen M. et al. “Sentinel Lesions of Primary CNS Lymphoma. J Neurol Neurosurg Psychiatry. 1996; 60: 102-105.