
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Unilateral absence of ovary and fallopian tube
Dan-Dan Wang; Ning-Ning Zhang; Qing Yang; Jiao Wang*
Department of Obstetrics and Gynecology, Shengjing Hospital of China Medical University, Shenyang, China.
*Corresponding Author : Jiao Wang
Department of Obstetrics & Gynecology, Shengjing
Hospital of China Medical University, No. 36 Sanhao
Street, Heping District, Shenyang, 110004, China.
Email: 785097813@qq.com & wangjiao881130@163.com
Received : Apr 05, 2021
Accepted : Apr 30, 2021
Published : May 05, 2021
Archived : www.jcimcr.org
Copyright : © Wang J (2021).
Citation: Wang DD, Zhang NN, Yang Q, Wang J. Unilateral absence of ovary and fallopian tube. J Clin Images Med Case Rep. 2021; 2(3): 1110.
Description
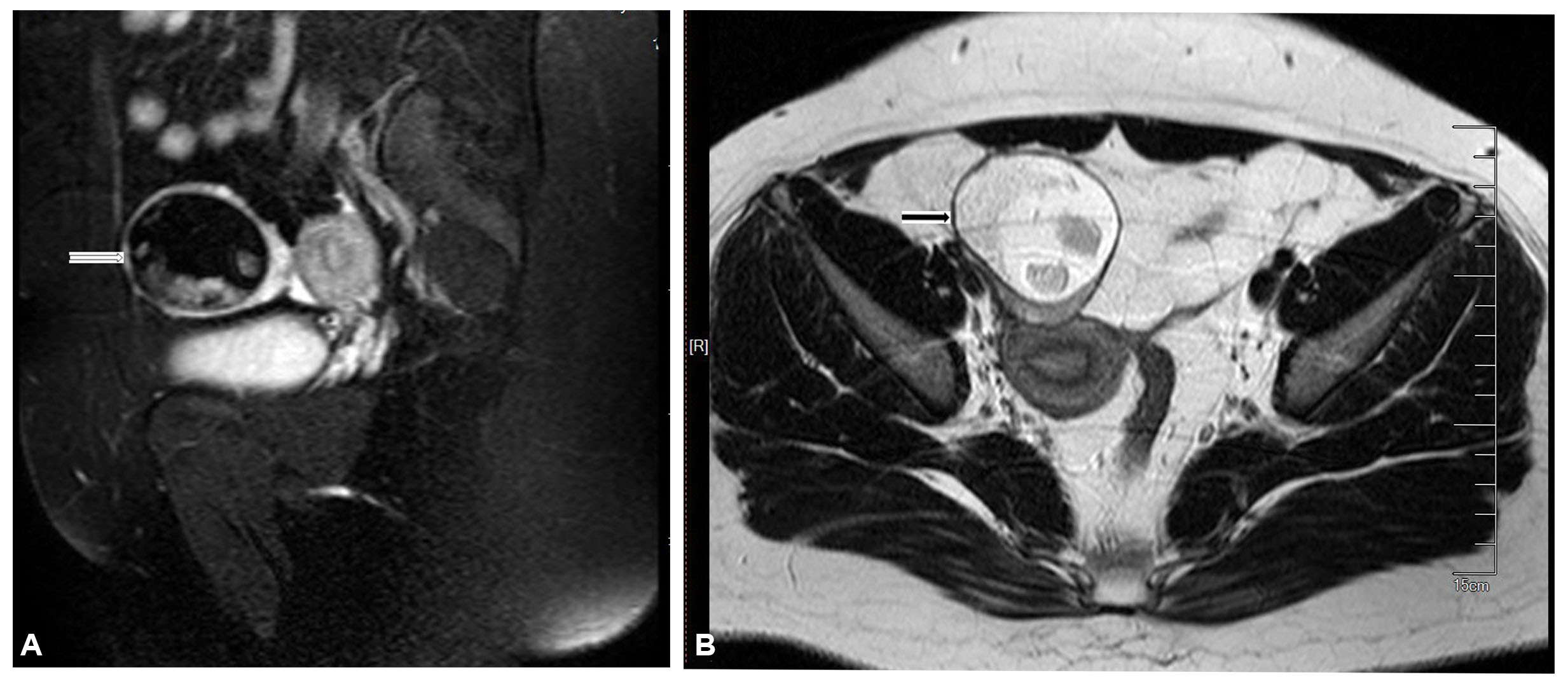
A 19-year-old young woman was admitted to our Unit for irregular menstrual cycles within 40- to 60-day intervals for 7 months. She had no history of abdomino-pelvic surgery or acute pelvic pain. Pelvic magnetic resonance imaging revealed a right ovarian mass (Figure1A & B), measuring 6.0 cm X 5.1 cm X 5.0 cm.
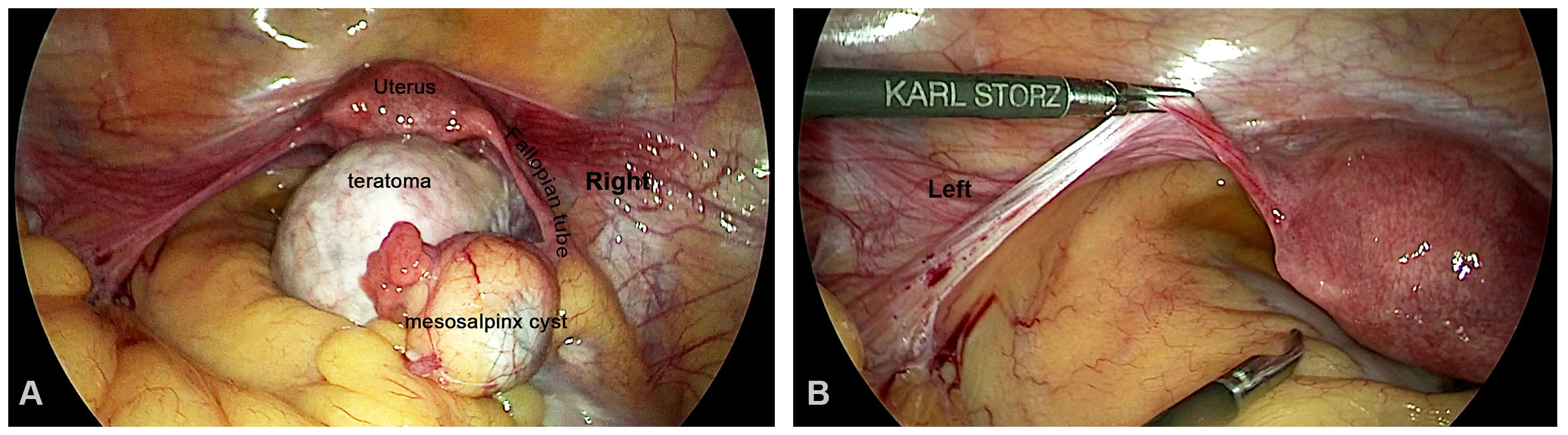
The patient underwent laparoscopy. At the laparoscopic examination, we evidenced a right ovarian teratoma about 6.0 cm X 6.0 cm and a small mesosalpinx cyst about 2.5 cm X 2.0 cm on the right fallopian tube (Figure 2A). On the left, neither fallopian tube nor ovary was detected (Figure 2B). We performed laparoscopic cystectomy and sutured residual ovarian tissues for hemostasis. Subsequent urinary ultrasonography demonstrated a normal urinary tract without any congenital anomaly. The pathological examination confirmed the diagnosis of mature teratoma and right mesosalpinx serous cyst. The patient was successfully discharged at the third day with no complications.
Partial or complete absence of unilateral ovary and fallopian tube is a rare occurrence, and the true etiologies remain unclear. Two possible hypotheses might be responsible [1-3]: (1) adnexal torsion (2) a defect in the development of the Mullerian and mesonephric system, either entirely or localized on one side of the genital ridge and the caudal part. Neither of the hypotheses could explain all of the sporadic cases reported to date. In the present case, the lack of other associated malformations makes the hypothesis of congenital defect unlikely, though no history of abdominal pain, the absence of unilateral ovary and tube does not exclude the possibility of a torsion that had occurred during fetal life.
Acknowledgements
This article was supported by Grants from the 345 Talent Project (30C) of Shengjing Hospital of China Medical University (No.14).
Declaration of patient consent: Written informed consent was obtained from the patient for publication of the case report and accompanying images.
Ethics committee approval: The study was approved by the institutional ethical board.
References
- Sivanesaratnam V. Unexplained unilateral absence of ovary and fallopian tube. Eur J Obstet Gynecol Reprod Med. 1986; 22: 103- 105.
- Uckuyu A, Ozcimen EE, Sevinc Ciftci FC. Unilateral congenital ovarian and partial tubal absence: Report of four cases with review of the literature. Fertil Steril. 2009; 91: 936.
- Pabuccu E, Kahraman K, Taskin S, Atabekoglu C. Unilateral absence of fallopian tube and ovary in an infertile patient. Fertil Steril. 2011; 96: e55-57.