
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Renal tubular injury as an uncommon presentation of Wilson’s disease
Hadar Mudrik-Zohar1,3*; Keren Cohen-Hagai2,3; Danny Alon1,3
1 Department of Internal Medicine, Meir Medical Center, Kfar Saba, Israel
2 Department of Nephrology and Hypertension, Meir Medical Center, Kfar Saba, Israel.
3 Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
*Corresponding Author : Hadar Mudrik-Zohar
Meir Medical Center, Tchernichovsky St 59, Kfar Saba
4428164, Israel.
Email: Hadar.mudrik@gmail.com
Received : Apr 04, 2021
Accepted : Apr 30, 2021
Published : May 05, 2021
Archived : www.jcimcr.org
Copyright : © Mudrik-Zohar H (2021).
Abstract
Wilson's disease is an autosomal recessive disorder caused by a mutant ATP7B gene on chromosome 13. This mutation causes a reduction in hepatic copper excretion, which accumulates in hepatocytes and deposits in other tissues and organs (brain, cornea, kidney, etc.) as the disease progresses.
Wilson's disease was described worldwide, with estimated prevalence of one case per 30,000 live births. Age of presentation is usually 4-60 years; however, the disease may present at any age. Clinical manifestations are predominantly hepatic, neurologic and psychiatric. Renal involvement is less common and characterized by proximal tubular dysfunction, Glomerular Filtration Rate (GFR) decline, renal tubular acidosis, aminoaciduria and nephrolithiasis.
Herein, we aimed to report a case which describes an uncommon path to the diagnosis of this rare, yet well-known disease. The diagnosis resulted from an investigation of acute kidney injury in a 48-year-old man.
Keywords: Wilson’s disease; Acute kidney injury; Renal tubular injury.
Citation: Mudrik-Zohar H, Cohen-Hagai K, Alon D. Renal tubular injury as an uncommon presentation of Wilson’s disease. J Clin Images Med Case Rep. 2021; 2(3): 1111.
Case report
A 48-year-old man with type 2 diabetes mellitus presented to our department with an acute kidney injury. He had no history suggesting hypovolemia, infection, nephrotoxic drugs or substance use or urinary obstruction. Physical examination was normal; however, bizarre behavior was noted. Laboratory tests revealed a new increase in creatinine level (3.5 mg/dL), elevated urea (215.0 mg/dl) and hyperchloremic metabolic acidosis. Liver enzymes and synthetic liver function were normal, except for a minimal increase in cholestatic enzymes. Urinalysis revealed 204.0 mOsm/kg osmolality, erythrocyturia, leukocyte sediments and pH persistently above 5.5. Kidney imaging ruledout obstructive uropathy. Laboratory test results for rheumatological and hematological disorders were also normal.
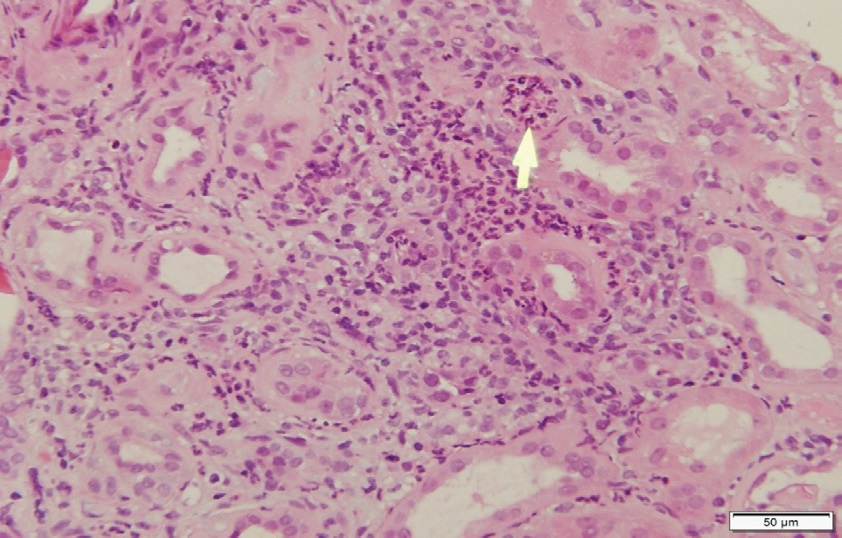
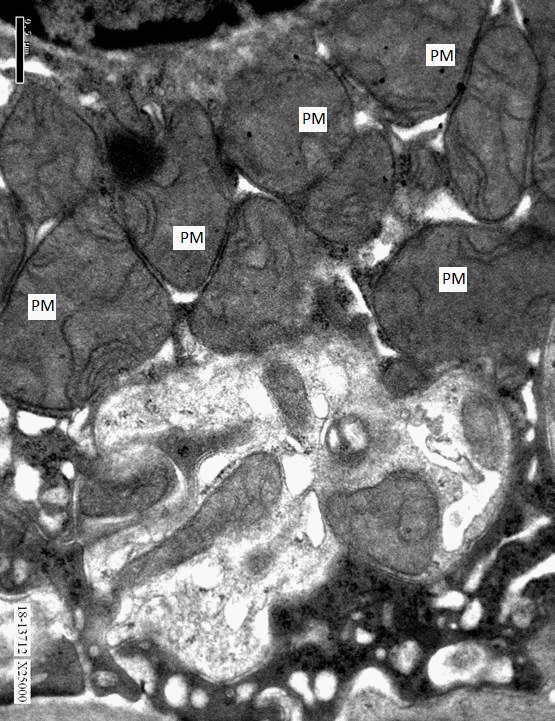
The patient was polyuric with a water deprivation test supporting partial-nephrogenic-diabetes insipidus and metabolic acidosis continued despite improvement in kidney function following hydration. Kidney biopsy was performed and revealed proximal-tubular injury (Figure 1) with dysmorphic mitochondria (Figure 2), alongside chronic interstitial injury (Figure 1).
The findings of our investigation suggested a possible diagnosis of Wilson’s disease, based mainly on kidney biopsy results, elevated cholestatic liver enzymes and the patient’s bizarre behavior, which developed progressively over several years according to heteroanamnesis.
We continued our investigation by measuring serum free copper which was elevated and serum ceruloplasmin which was normal, not low as expected, possibly explained by kidney failure. The patient’s urinary copper (24hr collection) was elevated (66 mcg/24 Hr) and a Kayser-Fleischer ring was found by ophthalmologist. No signs of hemolysis were found. Liver biopsy revealed increased copper deposition with no signs of cirrhosis. The patient was diagnosed using the Leipzig score (6 points) [1].
Discussion
Renal involvement in Wilson's disease is characterized by proximal tubular dysfunction, GFR decline, renal tubular acidosis and nephrolithiasis [2]. Glomerular injury was also described but is extremely rare. The tubular injury might be reversible with treatment [3]. Patients with Wilson's disease are known to have excessive urinary excretion of copper, and other manifestations of tubular injury such as aminoaciduria, glycosuria and uricosuria [4].
Diagnosing this 48-years old patient with Wilson's disease was not straightforward. While late-onset disease was previously described [5], at first, our only suggestive clues were his acquired cognitive impairment, the elevated cholestatic liver enzymes and the obvious proximal tubular injury. Furthermore, the patient's serum ceruloplasmin was normal, and not low as expected. Ceruloplasmin is normal in 10% of affected patients, and in this case, may be explained by advanced kidney failure [6]. The proximal-tubular injury and the dysmorphic mitochondria seen in Figures 1 and 2, suggested the possible diagnosis of Wilson's disease and by that, were the key for revealing the etiology of the kidney injury of our patient.
Conclusion
While renal involvement in Wilson's disease is well described, diagnosing the disease while investigating acute kidney injury of unclear etiology is highly uncommon. This rare disease should be suspected in patients with proximal tubular dysfunction without known etiology in the proper clinical setting.
Acknowledgements: We would like to thank Dr Yona KitayCohen, Dr Tania Zehavi and Dr Andrew Eyre from the Liver Clinic, the Pathology Institute and the Department of Internal Medicine A, respectively, at Meir Medical Center, Kfar Saba, Israel, for their helpful contributions.
References
- Ferenci P, Caca K, Loudianos G, Mieli‐Vergani G, Tanner S, Irmin S et al. Diagnosis and phenotypic classification of Wilson disease. Liver Int. 2003; 23: 139-142.
- Bearn AG, Yü TF, Gutman AB. Renal function in Wilson’s disease. J. Clin. Invest. 1957; 36: 1107.
- Evering WE, Haywood S, Elmes ME, Jasani B, Trafford J. Histochemical and immunocytochemical evaluation of copper and metallothionein in the liver and kidney of copper-loaded rats. J. Pathol. 1990; 160: 305-312.
- Elsas LJ, Hayslett JP, Spargo BH. Wilson’s disease with reversible renal tubular dysfunction: Correlation with proximal tubular ultrastructure. Ann Intern Med. 1971; 75: 427–433.
- Žigrai M, Vyskočil M, Tóthová A, Vereš P, Bluska P, et al. LateOnset Wilson’s Disease. Front. Med. 2020; 7.
- Yüce A, Koçak N, Ozen H, Gürakan F. Wilson’s disease patients with normal ceruloplasmin levels. Turk J Pediatr. 1999; 41: 99- 102.
- Zischka H, Lichtmannegger J, Schmitt S, Jägemann N, Schulz S, et al. Liver mitochondrial membrane crosslinking and destruction in a rat model of Wilson disease. J Clin Invest. 2011; 121: 1508–1518.