
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
What is your diagnosis? Labial adhesions – Classification and treatment
Giridhar Guntreddi*; Jayasree Vasudevan Nair; Swayam P Nirujogi
Sanford Medical Center, 1300 Anne St NW, Bemidji, MN 56601, USA.
*Corresponding Author : Giridhar Guntreddi
Sanford Medical Center, 1300 Anne St NW, Bemidji,
MN 56601, USA.
Email: guntreddig@yahoo.com
Received : Apr 05, 2021
Accepted : Apr 30, 2021
Published : May 05, 2021
Archived : www.jcimcr.org
Copyright : © Guntreddi G (2021).
Abbreviations: LA: Labial Adhesions; UTI: Urinary Tract Infection; Premarin cream.
Citation: Guntreddi G, Nair JV, Nirujogi SP. What is your diagnosis? Labial adhesions – Classification and treatment. J Clin Images Med Case Rep. 2021; 2(3): 1112.
Short report
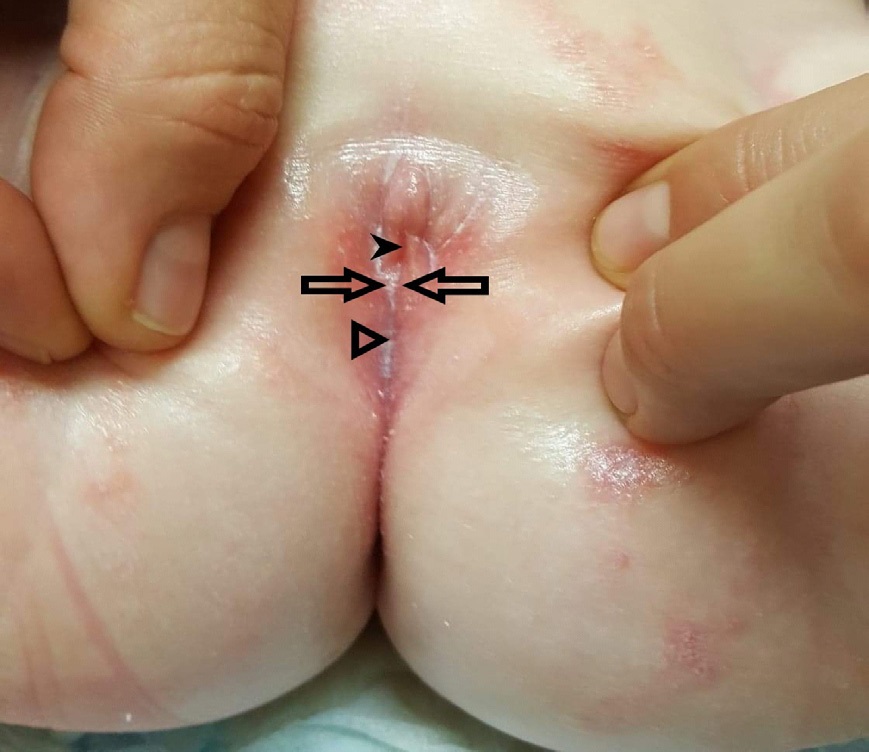
An 8-month-old Caucasian female infant with a history of two urinary tract infections presented with fever, poor oral intake, and increased irritability for 3 days prior to presentation. The mother reported a fever T max 103F and a strong odor of urine. Mother denied any cold, cough, diarrhea, vomiting, rash, and sick contacts at home. Her initial vitals were normal other than a temperature of 101F. The infant was alert, active and comfortable in her mother’s lap. On examination of her external genitalia, there was fused labia minora at the midline forming a midline raphe, and pinhole urethral opening was also noted (Figure 1). Due to close approximation of labia minora and tiny urethral opening, we were unbale to catheterize the bladder. According to the mother, previous attempts to catheterize the bladder for urinary samples were never successful as well. We confirmed the labial adhesions as shown in (Figure 1) based on our clinical examination and a presumptive diagnosis of UTI was made based on a positive bag urine sample and her symptoms.
Labial adhesions/vulvar synechiae (Figure 1) are defined as fusion of the Labia minora in the midline. It is one of the most common pediatric-gynecological problems [1] with an estimated prevalence of 0.6 to 5%, with a peak incidence between 13 to 23 months of age [2]. Chronic inflammation of the labia minora combined with the hypoestrogenic state of the female infant is considered as the possible explanation of the condition. The labia minora stick together in the midline, usually from posterior to forwards until only a small opening is left anteriorly through which urine is passed and present as labial adhesions. Other contributory factors are poor perineal hygiene, vulval irritation, chronic diaper use, and sexual abuse [3]. Vaginal infections with candida, group A streptococcus, Gonorrhea, Gardnerella vaginalis, chlamydia trachomatis, and trichomonas vaginalis are also considered as etiological factors in the environment of low estrogenic state.
LA is usually asymptomatic and is detected incidentally by a meticulous examiner/parents. They may present as post void dribbling, local irritation, vaginal pain, or discharge, recurrent UTI’s or rarely urinary retention [4]. There is a midline area of clear, fibrotic tissue at the site of adhesion, referred to as the raphe (Figure 1). Labial adhesions are divided into four types [5] depending on the amount and type of fusion.
a. LA Type 1 (48%): Fusion tissue is translucent and thin and can be separated by minor traction of labial folds during exam. The reflections of the hymen and other vestibular structures can be easily visualized behind the thin and translucent line of adhesion [5].
b. LA Type 2 (20%): Fusion tissue is thick. The reflection of the hymen and other vestibular structures cannot be visualized.
c. LA Type 3 (24%): Fusion tissue is thick. The reflection of the vulval components cannot be visualized. Distinguishing feature is that the hymen is slightly adherent to the labia minora [5].
d. LA Type 4 (8%): Fusion area is lateralized to the right or left side and not located in the midline. In these patients’ adhesion occurs when one labia minora adheres to the inner surface of the other.
Asymptomatic patients with a minor extent or labial adhesions less than 50% of the length do not require treatment [6]. Symptomatic patients (type 1 and type 2) need topical estrogen (Premarin vaginal cream or Estradiol 0.01% vaginal cream). It should be applied on midline raphe with Q tip or finger, once a day for at least 2 to 12 weeks. Topical 0.05% Betamethasone is used for recurrent adhesions or for failed treatment with topical estrogen. A 67%-95% success was observed with twice daily application of Betamethasone for 4 to 6 weeks [7]. Recurrence or treatment failure in type 3 and type 4 LA patients require manual or surgical separation. After surgery, they are supposed to be treated with daily topical estrogen for 2 to 4 weeks [8], followed by bland emollients for several weeks.
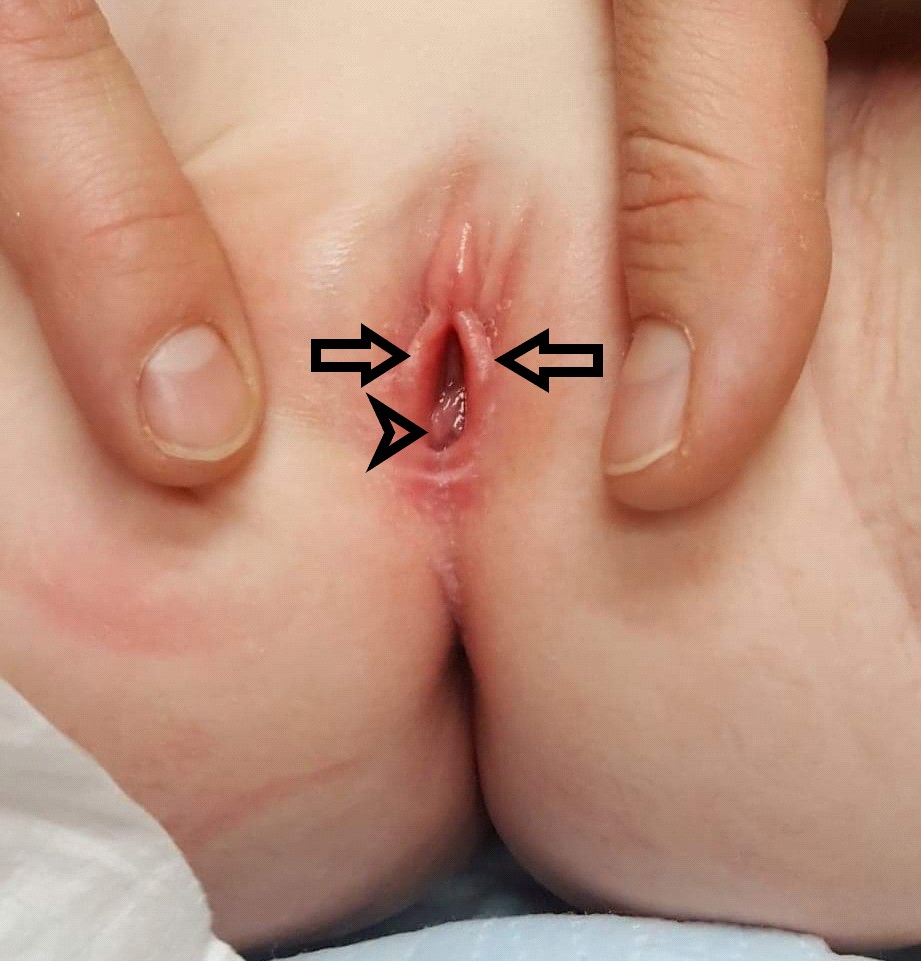
Our patient was diagnosed with type 2 labial adhesions. She was treated with oral Keflex for 7 days for UTI and topical Premarin vaginal cream for 4 weeks for labial adhesions. She responded nicely with complete separation of labia minora with clear visualization of vaginal introitus (Figure 2). So far, no recurrence of LA noted at her 6 months follow-up visit. She did not have any further urinary tract infections and her renal ultrasound was unremarkable.
LA is a common reason for consultation with pediatric gynecology. Thorough physical exam including genital exam is highly advocated for early and accurate diagnosis of the type of adhesions followed by appropriate treatment and follow up. Educating the parents about the etiology, treatment options and the chances of possible recurrence of this clinical entity along with age adjusted hygienic measures are highly recommended.
References
- Edmonds DK. Normal and abnormal development of the genital tract. In Edmonds DK, editor. Dewhurst’s Textbook of Obstetrics and Gynecology. 8th ed. UK: Blackwell publishing. 2012; 421- 434.
- Gibbon K, Bewley A, Salisbury J. Labial fusion in children: A [resenting feature of genital Lichen sclerosus? Pediatric Dermatol. 1999; 16: 388.
- Bacon JL, Romano ME, Quint EH. Clinical recommendation: Labial adhesions. North American society for pediatric and Adolescent Gynecology. Published by Elsevier Inc. 2015.
- Norbeck J, Ritchey M, Bloom D. Labial fusion causing upper urinary tract obstruction. Urology. 1993; 42; 209-211.
- Huseynov M, Hakalmaz AE. Labial adhesion; New classification and treatment protocol. North American society for Pediatric and Adolescent Gynecology. Published by Elsevier Inc. 2020; 33: 343-348
- Laufer MR, Means SJ. Vulvovaginal complaints in the prepubertal child. 2017.
- Muram D. Treatment of prepubertal girls with labial adhesions. J. pediatric Adolescent Gynecol. 1999; 12: 67.
- Soyer T. Topical estrogen therapy in labial adhesions in children: therapeutic or prophylactic? J. pediatr Adolesc Gynecol. 2007; 20: 241.