
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Evaluation of the morphometric relationship between the alveolar bone and gingival dimensions in the maxillary anterior teeth using cone-beam computed tomography imaging: A cross-sectional study
Katia Montanha-Andrade1; Ieda M Crusoé-Rebello2; Nara Santos Araujo1; Maurício Andrade Barreto3; Jean Nunes dos Santos4; Patricia R Cury5*
1 Post-graduate Program in Dentistry and Health, School of Dentistry, Federal University of Bahia, Salvador, Brazil.
2 Division of Dentomaxillofacial Radiology, School of Dentistry, Federal University of Bahia, Salvador, Brazil.
3 Associate Professor, Division of Implantology, Bahiana School of Medicine and Public Health, Salvador, Brazil.
4 Division of Oral Pathology, School of Dentistry, Federal University of Bahia, Salvador, Brazil.
5 Associate Professor, Division of Periodontics, School of Dentistry, Federal University of Bahia, Salvador, Brazil.
*Corresponding Author : Patricia Ramos Cury
School of Dentistry, Federal University of Bahia, Av.
Araújo Pinho, 62, Canela 40110-150, Salvador/Bahia,
Brazil.
Email: patcury@yahoo.com
Received : Apr 05, 2021
Accepted : Apr 30, 2021
Published : May 05, 2021
Archived : www.jcimcr.org
Copyright : © Cury PR (2021).
Abstract
The purpose of this study was to investigate the relationship between the alveolar bone and gingival dimensions in the maxillary anterior teeth. Cone-beam computed tomography images of 160 maxillary anterior teeth were evaluated. The Bone (BT) and Gingival Thickness (GT) and distances between Cemento-Enamel Junction (CEJ) and alveolar Bone Crest (CEJ-BC) and Cemento-Enamel Junction and Gingival Margin (CEJ-GM) were measured on the labial surface at the cervical third of the tooth root. Pearson correlation test or partial correlation was used. BT was significantly and positively associated with CEJ-GM in lateral incisors (p=0.04). The correlation between CEJBC and CEJ-GM was negative and statistically significant for incisors and canines (p≤0.01). The correlation between CEJ-BC and GT was positive and statistically significant for central incisors and canines (p≤0.01). Greater bone thickness was associated with higher gingival margin level at the lateral incisor, but not with bone crest level. Lower bone crest level was associated with greater gingival thickness at the central incisor and canines, and with lower gingival margin level at all the anterior maxillary teeth. The planning of orthodontic, periodontal, and restorative treatments should consider these dimensions of marginal periodontal tissue are interrelated and their relationship vary by tooth type.
Keywords: Alveolar process; Anatomy; Cone-beam computed tomography; Gingiva; Humans.
Citation: Cury PR, Montanha-Andrade K, Crusoé-Rebello IM, Araujo NS, Barreto MA. Evaluation of the morphometric relationship between the alveolar bone and gingival dimensions in the maxillary anterior teeth using cone-beam computed tomography imaging: A cross-sectional study. J Clin Images Med Case Rep. 2021; 2(3): 1113.
Introduction
The anatomy and relationships of the gingival tissue and underlying alveolar bone are important aspects to consider during dentistry planning as they influence the treatments outcome [1-7].
Studies investigating the relationship between bone and gingival dimensions have reported conflicting results (Table 1) [1- 9]. The associations of bone thickness and alveolar bone crest or gingival margin levels remain unclear and may impact gingiva recession development.
Table 1: In vivo study on the relationship between alveolar bone and gingival dimensions in maxillary anterior teeth
Reference |
Sample |
Measurement Methods |
Results |
Cook et al. [1] |
N=60 individuals (360 maxillary anterior teeth) |
Periodontal biotype and GR: clinical examination and periodontal probe transparency |
Thin biotype correlated with < BT, and with > CEJ-BC |
La Rocca et al. [2] |
N=15 individuals (180 maxillary and mandibular anterior teeth) |
GT: periodontal probe BT: CBCT |
No correlation between BT and GT |
Stein et al. [3] |
N= 60 individuals (60 left central incisors) |
Gingival and alveolar bone dimensions: parallel profile radiographs |
Correlation between BT and GT |
Nikiforidou et al. [4] |
N=42 individuals (186 maxillary and mandibular anterior teeth) |
BT, GT, CEJ-BC, BC-GM: CBCT |
Correlation between BT and GT, GT and CEJ-BC, GT and BC-GM, CEJ-BC and BC-GM |
Younes et al. [5] |
N=21 individuals (maxillary anterior teeth) |
GT: ultrasonic device BT: CBCT |
Correlation between BT and GT |
Amid et al. [6] |
N= 144 individuals (621 maxillary anterior teeth) |
BT, GT, CEJ-BC: CBCT |
Correlation between BT and GT (central and lateral incisor; no in canines). |
Da’Silva et al. [7] |
N=66 individuals (363 anterior maxillary teeth) |
BT, GT, BC-GM, CEJ-BC: CBCT |
Correlation between BT and GT, BC-GM and GT, CEJ-BC and BC-GM, BT and GR |
Kim et al. [8] |
N= 20 individuals (126 maxillary anterior teeth) |
CBCT and intraoral scanned soft tissue |
No correlation between BT and GT |
GR: Gingival Recession; GT: Gingival Thickness; BT: Bone Thickness; CEJ: Cemento-Enamel Junction; BC: Bone Crest; CBCT: Cone Beam Computed Tomography.
Considering previous studies’ limitations, additional research is needed. The aim of this study was to investigate the relationship between the alveolar bone crest and gingival dimensions in the maxillary anterior teeth using Cone-Beam Computed Tomography (CBCT).
Material and methods
The study was approved by the Ethical Committee of XXXXXXX (Protocol number: 1.759.719) and conducted according to the tenets of the Declaration of Helsinki.
Study design, setting, and participants
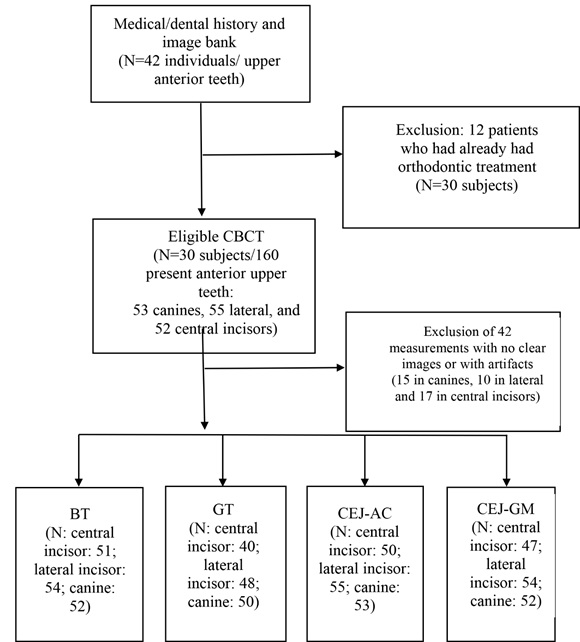
This cross-sectional study included a convenience sample of 30 individuals with 160 teeth: 52 central incisors, 55 lateral incisors, and 53 canines. A total of 42 patients were screened by these inclusion and exclusion criteria, but twelve were excluded due to previous orthodontic treatment. Twenty maxillary anterior teeth were missing in the selected patients (Figure 1).
BT, GT, and CEJ-BC and CEJ-GM distance were considered as the primary outcomes. GM-BC distance was considered as the secondary outcome. Sex and age were treated as potential confounders.
A CBCT image database of patients who underwent CBCT as a diagnostic procedure between January, 2017 and March, 2019 was searched according to the following inclusion criteria: Patients with available images of the upper anterior teeth and of age 18 years and older.
The exclusion criteria were
1. Previous orthodontic treatment or malocclusion;
2. Endodontic pathology in the regions of interest;
3. Dental restorations exceeding beyond the cementoenamel junction (CEJ);
4. Dental shape abnormalities;
3. Radiographic findings of alveolar bone loss indicating
periodontitis;
4. Previous surgical intervention in the anterior maxillary region;
5. Pregnancy;
6. Use of medications that can induce gingival growth;
7. Systemic diseases that can affect periodontal tissues, including acquired immunodeficiency syndrome, diabetes
mellitus, congenital disorders, and Crohn’s disease
CBCT scanning and analysis
At the time of CBCT scanning, a plastic lip retractor was placed in each patient’s mouth [10], and images were acquired using a tomography device (CS 8100 3D Unit; Carestream Health Inc., Marne La Vallée, France). The acquisition protocol was according to manufacturer’s recommendation and patient’s clinical indication, with a voxel size of 0.15 mm and field-of-view of at least 100 × 50 mm.
All measurements were performed using CS 3D Imaging software (version 3.5.18; Carestream Health Inc., Rochester, New York, USA) by a single examiner (KMA), who is an orthodontist with broad experience in CBCT, blinded to the patient’s clinical information or reference standard values. For the reliability-repeatability assessment, the examiner was trained by an experienced radiologist (IMCR) examining CBCT from 10 patients. The inter and intra-examiner concordance coefficient was > 0.8 for all linear measurements.
Visual assessment was conducted with adjustments in brightness, contrast, and zoom function.
Briefly, the tooth was centered in the three slices (axial, coronal, and sagittal) of CBCT images. The vertical angulation was set according to the long axis at the center of the tooth of interest and the horizontal angulation was set perpendicular to the alveolar ridge. Subsequently, a sagittal section was generated, and a horizontal reference line was made at the level of CEJ.
The distance between CEJ and the apex of the tooth was measured, and the tooth root was divided into three segments: cervical, middle, and apical. Next, using the horizontal reference line at CEJ, the CEJ-BC and GM-BC distances were determined. The BT and GT were measured at the center of the buccal region of the cervical third of the root (Figure 2). The CEJ-GM distance was computed by subtracting CEJ-BC from GM-BC. In 42 teeth, a few measurements could not be performed due to poor visualization of the bone, gingiva, or CEJ.
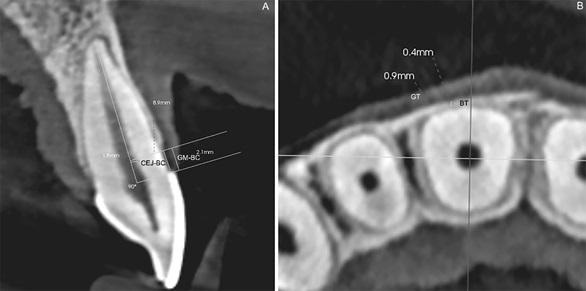
In each tooth, CEJ-BC and GM-BC were measured in the centered sagittal view, while BT and GT were measured in the axial view.
Statistical analysis
For 160 maxillary anterior teeth, analyses were conducted by omitting the missing measurements, with each tooth as an experimental unit.
Pearson correlation test was used to evaluate the association between the dimensions for each tooth group.
The significance threshold was set at α=0.05 and the Statistical package of social science program (SPSS version 13.0; SPSS Inc., Chicago, Illinois, USA) was used to analyze the data.
Results
General characteristics of the sample
A total of 160 maxillary anterior teeth from 30 individuals (19 females and 11 males) were included in the study. The patient age ranged from 18 to 66 years (mean ± standard deviation: 39.40 ± 12.06 years).
The mean dimensions for each tooth are shown in table 2.
Table 2: Bone and gingival dimensions (in mm) according to teeth (mean ± standard deviation).
Tooth |
BT |
GT |
CEJ-BC |
CEJ-GM |
GM-BC |
Central Incisors |
0.48 ± 0.20* |
0.62 ± 0.22* |
1.93 ± 0.68 |
1.05 ± 0.82 |
2.99 ± 0.88 |
Lateral Incisors |
0.46 ± 0.26* |
0.51± 0.27* |
2.10 ± 1.40 |
1.34 ± 1.24* |
3.44 ± 1.26 |
Canines |
0.35 ± 0.20 |
0.39 ± 0.19 |
2.33 ± 1.06 |
0.74 ± 1.11 |
3.07 ± 0.78 |
General |
0.43± 0.23 |
0.50 ± 0.24 |
2.12 ± 1.10 |
1.04 ± 1.09 |
3.17 ± 1.01 |
*: p ≤ 0.05 (compared to canines; Tukey test)
CEJ-BC was negatively correlated with CEJ-GM, and the correlation was statistically significant for the incisors and canines (p ≤ 0.01), indicating that higher levels of the gingival margin were associated with higher levels of the alveolar bone crest. A stronger correlation was observed in the canines (R=-0.74) than in the central incisors (R=- 0.33) and lateral incisors (R=-0.56) (Table 3).
Table 3: Correlation (R) between bone and gingival dimensions.
|
Coefficient the correlation (R) |
||
Dimensions |
Central Incisors |
Lateral Incisors |
Canines |
Distance from CEJ-BC: |
|
|
|
Bone thickness |
0.10 |
-0.17 |
-0.21 |
Gingiva thickness |
0.42** |
0.21 |
0.35* |
Distance CEJ-GM |
-0.33** |
-0.56** |
-0.74** |
Distance from CEJ-GM: |
|
|
|
Bone thickness |
0.19 |
0.28* |
0.12 |
Gingival thickness |
0.19 |
0.13 |
-0.11 |
Bone thickness x Gingiva thickness |
-0.10 |
0.04 |
-0.03 |
* p≤ 0.05 (Pearson Correlation test); ** p≤ 0.05 (Partial correlation test)
CEJ-BC was positively correlated with GT, and the correlation was statistically significant for the central incisors and canines (p ≤ 0.01), indicating decreased bone levels at greater thickness values of the gingiva.
CEJ-GM was significantly associated with BT at the lateral incisors (p=0.04), indicating greater thickness of the bone at higher levels of the gingiva.
No significant correlation was observed between GT and BT (p ≥ 0.75).
Discussion
The aim of this study was original, as any previous study evaluated the impact of bone thickness on crest bone and gingival heights. Moreover, considering the lack of consensus on the morphometric relationship between alveolar and gingival dimensions, additional studies were essential to understand this matter. The results mainly revealed that: 1) BT was associated only with CEJ-GM for the lateral incisors; 2) CEJ-BC was associated with GT for the central incisor and canines and with CEJ-GM for all teeth and; 3) the other bone and gingival dimensions were not associated. Therefore, the study’s hypothesis was partially confirmed.
One important strength of this study was the use of CBCT imaging. CBCT systems have been developed for imaging hard tissues of the maxillofacial region and provide the dental clinician with a three-dimensional representation of the mineralized tissues with minimal distortion. However, with the simple use of a plastic lip retractor and the retraction of the tongue toward the mouth floor during CBCT scanning, the soft tissue around the teeth can be discriminated in the images [10]. CBCT may be considered a non-invasive method, compared to bone sounding and transgingival probing, which have also been used to measure hard and soft tissue around the teeth and are performed under local anesthesia [5,12]. Nevertheless, the radiation dose delivered by CBCT may be considered a drawback. It is higher than the dose delivered by digital panoramic and intra-oral radiographs. The range of the effective dose for a panoramic radiograph is between 3.85 and 38.0 µSv and for one intra oral examination, between 0.65 and 9.5 µSv [13], while for CBCT examination it ranges from 61 to 134 µSv. Although effective dose of CBCT is several hundreds of times higher than the effective dose from conventional dental radiographic examinations, The Health Physics Society recommends against quantitative estimation of health risks below an individual dose of 50 mSv in one year, or a lifetime dose of 100 mSv [14]. Therefore, for CBCT, risks are either too small to be observed or are nonexistent.
In this study, the CEJ-BC value (bone level) was not associated with BT, which was unexpected as a greater bone thickness seems related to higher bone level [15]. To the best of our knowledge, no study has previously evaluated the relationship between CEJ-BC and BT, although this interrelation has been suggested in a study of alveolar bone anatomic profiles in dry skulls [15].
In the current study, the GM position was more coronal when the bone was thicker, but only in the lateral incisors, a relationship that has not been previously studied and it was presumed to be found for all anterior teeth. In consonance with this result, a positive association between clinically evaluated gingival recession and BT for all anterior teeth was recently reported [7]. Furthermore, contrary to what was expected and previously described [4,7], no association between GM position and GT was identified. In this study, it was not possible to measure CEJGM distance on the CBCT images for some teeth. On the other hand, it is not easy to identify CEJ using the clinical approach. Therefore, both methods have limitations, and the discrepancies between the studies may be related to differences in the methodology used. Further, studies are required to clarify the lack of association between GM position and bone thickness in central incisors and canine and between GM position and GT. However, in the present study, all tooth groups attained a more coronal position of GM when the bone level was more coronal. This result agrees with the conventional concept that morphologic characteristics of the gingiva are related to the dimensions of the alveolar process [4,7,15,16].
In the present study, the CEJ-BC distance was greater (lower bone level) when the gingival tissue was thicker, except at the lateral incisors, which contrasts with the findings of previous studies that the thin biotype was associated with a lower bone level [1,4]. Another study found no significant associations among these measurements for any tooth type [6]. The difference in results obtained can be explained by the fact that GT was measured using CBCT images by this investigation and by Amid et al. [6] and Nikiforidou et al. [4], whereas clinical examination was used to categorize the gingival tissues as either thick, average, or thin biotype by Cook et al. [1]. In addition, a single analysis was conducted for all the maxillary anterior teeth by Nikiforidou et al [4].
Moreover, the BT showed no association with GT, which conflicts with the result of a positive association between BT and GT in some studies [1,5,6] and agrees with the absence of association in other studies [2,8]. Many factors, including tooth inclination [17] and the CTCB protocol, can impact this relationship. The images were acquired using a 0.125-mm voxel size, compared to a voxel size between 0.2 and 0.4 mm used in some previous studies [2,5,6]. Although the standard diagnostic protocol is not available at this time, smaller voxels tend to yield more accurate results [18]. Investigators have used different methodologies to measure GT, including ultrasonic device [5], which is not reliable when the gingival thickness is greater than 0.5 mm [12];and probe transparency [1,2],which does not measure the gingival thickness but only discriminates between thin or thick according to probe transparency through the free gingiva [3].
This study had some limitations. First, the cross-sectional study design limits the understanding of the sequence of events and the causal relationships among the variables. Second, a small sample was included; although a power of ≥ 0.7 was calculated for the statistically significant associations, a power of < 0.6 was obtained for associations without statistical significance. Third, a few measurements could not be made in 42 teeth due to poor visualization of the bone, gingiva, or CEJ.
These results have clinical relevance related to the planning of orthodontic, periodontal and restorative treatments in anterior region of maxilla, especially when a CTCB imaging is not available. When planning orthodontic movement or periodontal flaps in areas showing lower gingival height, it would be expected a lower bone level, and in lateral incisors, a lower bone thickness as well. Therefore, the professional should be cautious during orthodontic movement and periodontal flap, as further bone loss is an undesirable outcome may compromise the treatments. In addition, although a thicker gingival margin has been considered more stable [19], it can be suggested that very thick gingival margin may jeopardize a satisfactory self-performed plaque control, which could result in a lower bone level and should be considered during periodontal surgeries. Finally, maximum attention is also demanded concerning the structures of the dentogingival attachment apparatus in the restorative treatment. Since bone and gingival levels were related to each other, a gingival recession following an esthetic rehabilitation invading the biological width would have negative esthetic impact. However, longitudinal studies are required to provide information on the cause-and-effect relationship between the bone and gingival dimensions and the clinical significance of the present results.
Conclusions
In conclusion, a greater bone thickness was associated with a higher gingival margin level at the lateral incisor, but not with bone crest level. Lower bone crest level was associated with greater gingival thickness at the central incisor and canines, and with lower gingival margin level at all the anterior maxillary teeth. Clinicians should be aware that the marginal periodontal tissue dimensions are interrelated, and the relationship varies according to the tooth type, when planning orthodontic, periodontal, and restorative treatment involving the anterior teeth.
Declarations
Conflicts of interest: The authors do not have any financial interest in the companies whose materials are included in this article.
Acknowledgements: The study was approved by the Ethical Committee of Bahiana School of Medicine and Public Health, Bahia, Brazil (protocol number: 1.759.719) and conducted according to the tenets of the Declaration of Helsinki.
References
- Cook DR, Mealey BL, Verrett RG, et al. Relationship between clinical periodontal biotype and labial plate thickness: An in vivo study. Int J Periodontics Restorative Dent. 2010; 31: 345–354.
- La Rocca AP, Alemany AS, Levi P, et al. Anterior maxillary and mandibular biotype: Relationship between gingival thickness and width with respect to underlying bone thickness. Implant Dent. 2012; 21: 507–515.
- Stein JM, Lintel-Höping N, Hammächer C, et al. The gingival biotype: Measurement of soft and hard tissue dimensions - A radiographic morphometric study. J Clin Periodontol. 2013; 40: 1132–1139.
- Nikiforidou M, Tsalikis L, Angelopoulos C, et al. Classification of periodontal biotypes with the use of CBCT. A cross-sectional study. Clin Oral Investig. 2016; 20: 2061–71.
- Younes F, Eghbali A, Raes M, et al. Relationship between buccal bone and gingival thickness revisited using non-invasive registration methods. Clin Oral Implants Res. 2016; 27: 523–528.
- Amid R, Mirakhori M, Safi Y, et al. Assessment of gingival biotype and facial hard/soft tissue dimensions in the maxillary anterior teeth region using cone beam computed tomography. Arch Oral Biol. 2017; 79: 1–6.
- D’Silva E, Fraser D, Wang B, et al. The association between gingival recession and buccal bone at maxillary anterior teeth. J Periodontol. 2019; 1–9.
- Kim YJ, Park JM, Kim S, et al. New method of assessing the relationship between buccal bone thickness and gingival thickness. J Periodontal Implant Sci. 2016; 46: 372–381.
- Kim DM, Bassir SH, Nguyen TT. Effect of gingival phenotype on the maintenance of periodontal health: An american academy of periodontology best evidence review. J Periodontol. 2020; 91: 311–338.
- Januário AL, Barriviera M, Duarte WR. Soft tissue cone-beam computed tomography: A novel method for the measurement of gingival tissue and the dimensions of the dentogingival unit. J Esthet Restor Dent. 2008; 20: 366–373.
- Ghassemian M, Nowzari H, Lajolo C, et al. The Thickness of Facial Alveolar Bone Overlying Healthy Maxillary Anterior Teeth. J Periodontol. 2012; 83: 187–197.
- Savitha B, Vandana K. Comparative assessment of gingival thickness using transgingival probing and ultrasonographic method. Indian J Dent Res. 2005; 16: 135–139.
- Li G. Patient radiation dose and protection from cone-beam computed tomography. Imaging Sci Dent. 2013; 43: 63-69.
- Health Physics Society. Position statement of the Health Physics Society. Radiation risk in perspective. 2011.
- Zweers J, Thomas R, Slot D et al. Characteristics of periodontal biotype, its dimensions, associations and prevalence: A systematic review. J Clin Periodontol. 2014; 41: 958–971.
- Ochsenbein C, Ross S. A reevaluation of osseous surgery. Dent Clin North Am. 1969; 13: 87–102.
- Sendyk M, de Paiva JB, Abrão J, Rino Neto J. Correlation between buccolingual tooth inclination and alveolar bone thickness in subjects with Class III dentofacial deformities. Am J Orthod Dentofacial Orthop. 2017; 152: 66–79.
- Spin-Neto R, Gotfredsen E, Wenzel A. Impact of voxel size variation on CBCT-based diagnostic outcome in dentistry: A systematic review. J Digit Imaging. 2013; 26: 813–20.
- Siebert J, Lindhe J. Textbook of Clinical Periodontology and Implant dentistry. 2nd ed. Copenhangen: Munksgaard. 1989.