
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Cryoablation of osteoid osteoma with hip traction
Nicolas Stacoffe1*; Damien Heidelberg1; Joris Lavigne2; Jean-Baptiste Pialat1,3
1 Service de Radiologie Groupement Hospitalier Sud, Hospices Civils de Lyon, Pierre-Bénite, France.
2 Service de Radiologie Groupement Hospitalier Centre, Hospices Civils de Lyon, Lyon France.
3 Université Claude Bernard Lyon 1 Lyon, Lyon, France.
*Corresponding Author : Nicolas Stacoffe
Service de Radiologie, Groupement Hospitalier Sud,
165 Chemin du Grand Revoyet, 69310 Pierre-Bénite,
France.
Email: nicolas.stacoffe@chu-lyon.fr
Received : Apr 05, 2021
Accepted : May 03, 2021
Published : May 06, 2021
Archived : www.jcimcr.org
Copyright : © Stacoffe N (2021).
Abstract
Benign tumors of the acetabular roof are a therapeutic challenge. Percutaneous ablations avoid complicated surgery. These tumors are close to the cartilage and therefore there is a risk of damaging and causing chondropathy. We propose here the case of an osteoid osteoma treated by cryobablation associated with a hip traction with arthro-CT with warmed serum.
Keywords: Cryoablation; Hip-traction; Osteoid osteoma; Mini-invasive; Interventional radiology
Citation: Stacoffe N, Heidelberg D, Lavigne J, Pialat JB. Cryoablation of osteoid osteoma with hip traction. J Clin Images Med Case Rep. 2021; 2(3): 1114.
Introduction
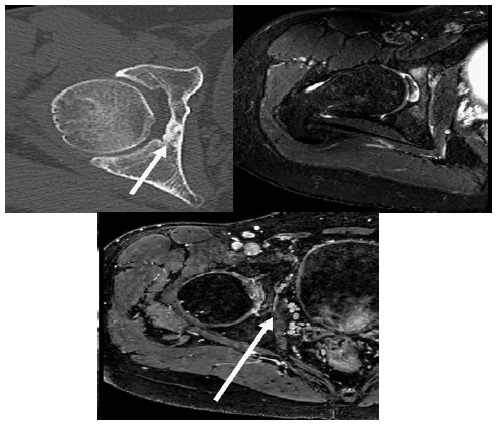
A 30-year-old man who sustained radiofrequency ablation for an osteoid osteoma two years ago presented pain reappearance of his right hip. The clinical presentation was suggestive of a recurrence of the osteoid osteoma. CT scan showed a persistent heterogeneous sclerotic lesion of the quadrilateral lamina (Figure 1a). MRI showed substantial inflammation surrounding the lesion and dynamic-enhanced sequences (DCE-MRI) revealed a focal spot with early hypervascuarization (Figure 1b & 1c). The location was closed to the acetabular and femoral head cartilage. In order to limit the risk of chondromalacia induced by the procedure, the cryoablation was preferred [1]. We also planned to protect the nearby cartilage by using warmed saline solution and hip traction during the ablation, because as a second treatment attempt, the ablation zone needed to be large enough.
Case presentation
The patient was settled in a supine position on the scanner table and sedated by the anesthesiologist. A locating helix was performed to target the focal lucency corresponding to the hypervascularized spot showed by the DCE-MRI [2].
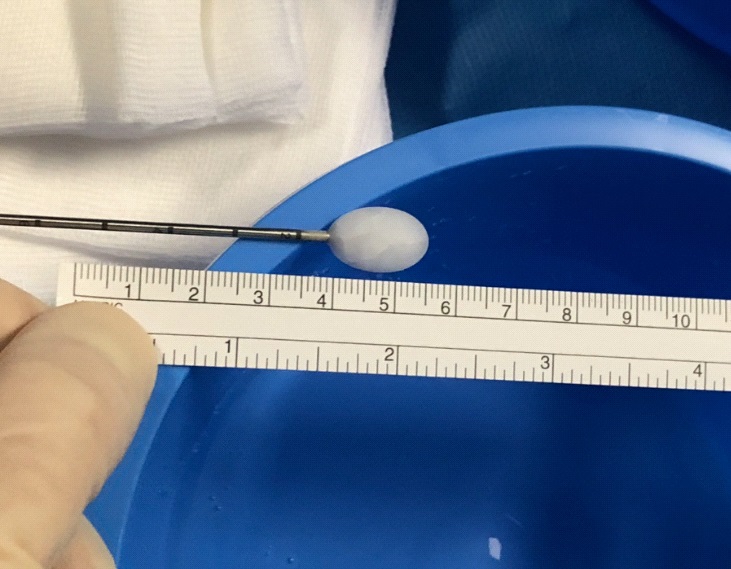
The anterior approach was chosen with hydrodissection between the femoral vessels and the spermatic chord [3]. A 13 gauges trocar was used to penetrate the bone and the bone path was made within the quadrilateral lamina using a 17 gauges bone biopsy needle up to the nidus. The bone biopsy needle was removed and replaced by the cryode (Cryoprobe PCS-17R, Endocare) after an ex-vivo ice-ball testing was made. To cover the lesion with sufficient margins, we decided to aim for a 15 mm length and 10 mm diameter ice-ball, using the cryode at 60% of its full power (Figure 2).
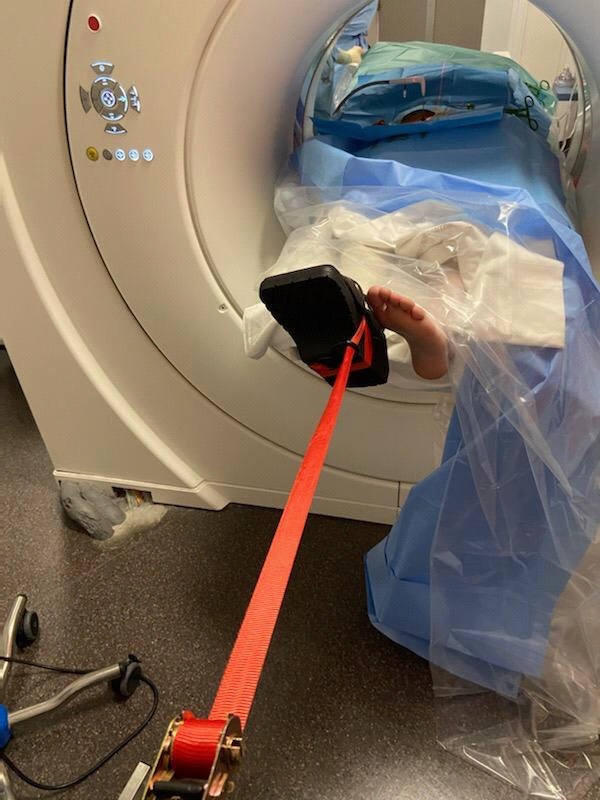
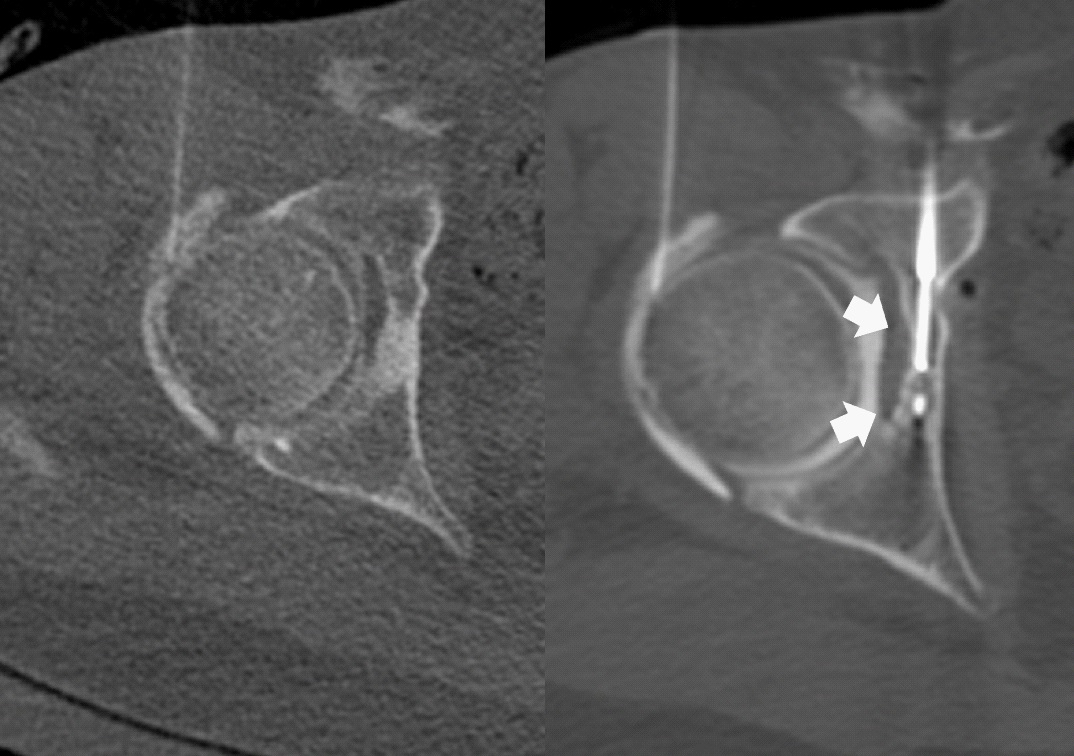
Before starting the treatment, we introduced a 22 gauges needle in the hip and injected 15 cc of warmed saline solution mixed with 5% diluted iodine contrast. The traction was carried out using a Barouk shoe hooked to a standard strap with a tension of 15 kgs (Figure 3). The hip decoaptation was verified on CT then we carried out two cycles of 10 minutes cryoablation at 60% power followed by 10 minutes of passive warming, respectively [4]. Between cycles, the hip liquid was aspired and replaced. The traction was paused in the five minutes before the second cycle and five minutes after the end of it. CT scan acquisitions were carried out at 9 minutes of each cycle, they showed persistent hip joint space enlargement due to the traction and correct positioning of the ball-ice distant to the articular cartilage (Figure 4a & 4b).
At the end of the procedure, the hip content was aspired, the cryode and trocar removed and the skin cleaned and closed with a sticky strip. The total procedure time was 90 minutes. The patient woke up with minor residual soreness at the site of puncture. Called two and six month later, he did not complain of any more pain.
Discussion/conclusions
Percutaneous treatments in interventional radiology have revolutionized the management of cancer patients in recent years. However, percutaneous means that we do not have visual access to the work area. In case of a lesion close to the joint, the risk is to make a cartilaginous lesion. In a multi-metastatic patient, we can take the risk which seems to be less than the benefit. On the other hand, in a young patient with a benign tumor such as an osteoid osteoma, we can ask ourselves the question of a secondary effect on the articular cartilage that will lead to secondary arthropathy in a few years. In our case, the arthro-CT with warmed serum injection and the traction allowed a good control of cartilage.
Combination of warm fluid injection and traction can be used to prevent cartilage injury when a cryoablation is performed nearby.
References
- Santiago E, Pauly V, Brun G, Guenoun D, Champsaur P, Le Corroller T. Percutaneous cryoablation for the treatment of osteoid osteoma in the adult population. Eur Radiol. 2018.
- Niazi GE, Basha MAA, Elsharkawi WFA, Zaitoun MMA. Computed tomography-guided radiofrequency ablation of osteoid osteoma in atypical Sites: Efficacy and Safety in a Large Case Series. Acad Radiol. 2020.
- Kostrzewa M, Henzler T, Schoenberg SO, Diehl SJ, Rathmann N. Clinical and Quantitative MRI perfusion Analysis of osteoid osteomas before and after Microwave ablation. Anticancer Res. 2019.
- Cerezal L, Carro LP, Llorca J, Fernandez-Hernando M, Llopis E, et al. Usefulness of MR arthrography of the hip with leg traction in the evaluation of ligamentum teres injuries. Skeletal Radiol. 2015.