
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
The role of bedside ultrasound during tracheal intubation procedure
José Luis Vázquez Martínez*; Rocío Tapia Moreno; César Pérez-Caballero Macarrón; Ana Coca Pérez; María Sánchez Porras; Diana Folgado Toledo
PICU, Universitary Ramón y Cajal Hospital, Madrid, Spain.
*Corresponding Author : José Luis Vázquez Martínez
PICU, Universitary Ramón y Cajal Hospital, Madrid,
Spain.
Email: jvazquez.hrc@salud.madrid.org
Received : Apr 03, 2021
Accepted : May 03, 2021
Published : May 06, 2021
Archived : www.jcimcr.org
Copyright : © Martínez JLV (2021).
Citation: Vazquez Martinez JL, Tapia R, Pérez-Caballero C, Coca A, Sánchez M, Folgado D. The role of bedside ultrasound during tracheal intubation procedure. J Clin Images Med Case Rep. 2021; 2(3): 1115.
Introduction
Tracheal intubation in complex settings (i.e. difficult airway, hemodynamic instability) means a challenging procedure [1]. It must be performed very quickly, being obviously essential to confirm the adequate positioning of the tube tip as soon as possible. Capnography is the most recommended tool in spite proper evaluation also includes clinical exam and X-ray, which implies some delay [2]. When capnography is not available and/ or misleading readings are present, bedside ultrasound can be extremely useful.
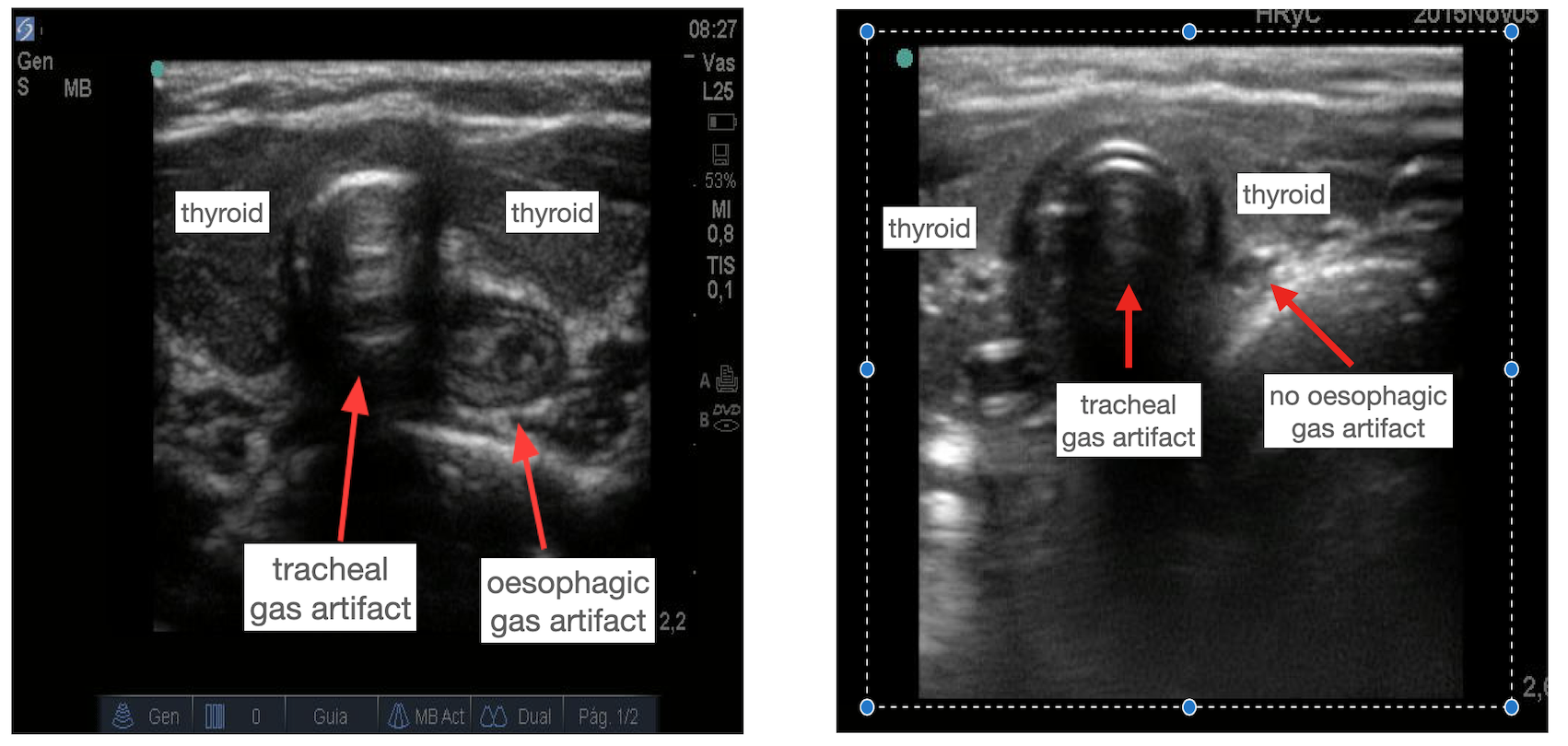
The T.R.U.E. (Tracheal Rapid Ultrasound Exam) protocol consists on performing transverse bedside upper airway ultrasonography, by placing a linear transducer over the suprasternal notch [3]. At this level, tracheal and oesophagus are easily identified. In case of unnoticed oesophageal intubation, a gas art fact emerges in the oesophagus lumen. To definitively confirm the optimal tracheal tube position, regardless the absence of oesophageal gas artifact, left lung sliding must be checked in order to rule in/out a selective bronchial intubation.
We show a case of failed tracheal intubation where clinical exam and capnography resulted inconclusive, and finally confirmed by bedside ultrasound.
Case description
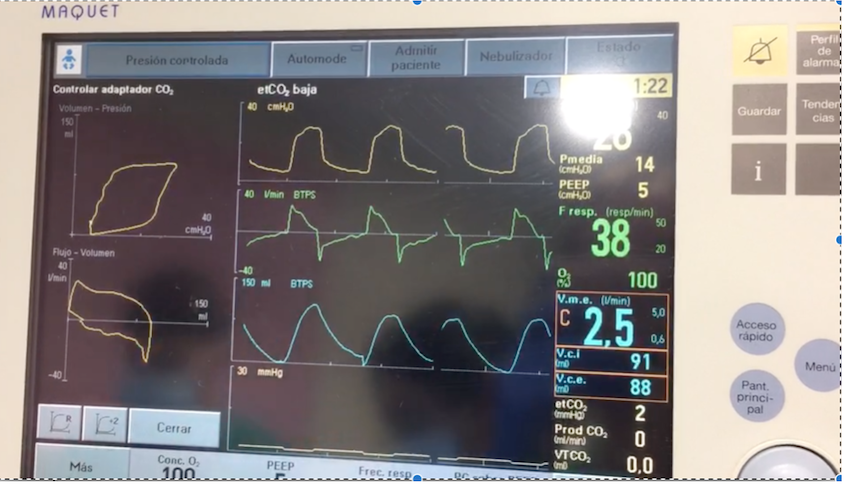
Infant one month old admitted to PICU because severe respiratory failure due to bronchiolitis, requiring emergent endotracheal intubation. The process resulted impaired because of absence of glottis visualization. After 3 failed attempts, a tracheal tube was seemingly well positioned: Thorax inspection showed adequate and symmetric inspiratory and expiratory movements meanwhile auscultation revealed normal lung sounds; pulse oximetric readings were sustained over 90% and capnography shared unstable readings (2-15 mmHg). Due to this fact, a malfunctioning capnography was suspected, thus the patient was connected to the ventilator and pressure/time and flow/time curves were assessed, corresponding all them to an adequate tracheal intubation (Figure 1).
An X-ray was performed in the time waiting for the X-ray visualization, TRUE protocol was also performed demonstrating oesophageal intubation (as gas artifact were both detected in the trachea and in the oesophageal lumen) (Figure 2).
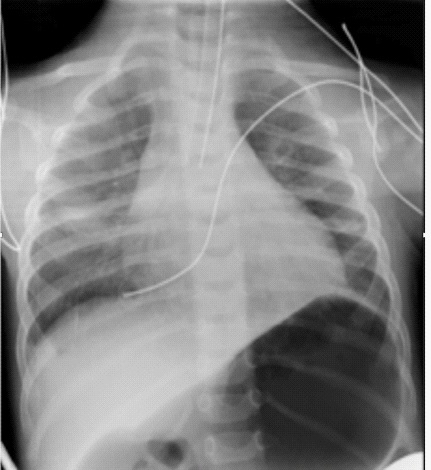
Interestingly enough, left lung sliding was presented. A new and successful intubation attempt was done, later confirmed either by ultrasound and by second X-ray (tube near the tracheal bifurcation and distended stomach because of previous ventilation through the oesophageal tube). (Figure 3).
Discussion
Considering the harm of misplaced tracheal tube, it is mandatory to immediately examine tube placement by bedside methods, such as capnography. In spite it is considered the gold-standard, it requires lung ventilation (meaning high risk of aspiration when oesophageal intubation) and could be malfunctioning leading to false positive (unfasted patients) or false negative results (i.e., because of the presence of water in the sampling line) [4]. Nowadays, bedside ultrasound emerges as an excellent point-of-care tool. After a short period of training, it is feasible and accurate in order to rule-in/out tracheal intubation by applying the T.R.U.E. protocol [5]. It can be rapidly performed (it takes no longer than 20 seconds in skilled hands) without interfering intubation maneuvers. Lung ventilation is just needed once the tube has been confirmed to be intratracheal in order to rule out a right main bronchi intubation.
Our case shows the feasibility of T.R.U.E. in children, too. Due to the delay between X-ray performance and X-ray report, ultrasound gave us crucial bedside and immediate information. Oddly enough, clinical exam and ventilator curves failed. Probably, the initial tube position was supraglottic; this fact plus the premedication with neuromuscular blockage allowed an adequate insufflation of both hemithorax with positive pressure ventilation, but unable to reach stable capnometry readings over 15 mmHg. In conclusion, we promote the use of bedside ultrasound during tracheal intubation procedure as a complementary method to assess the tube positioning.
References
- Zechner PM, Breitkreutz R. Ultrasound instead of capnometry for confirming tracheal tube placement in an emergency? Resuscitation. 2011; 82: 1259-1261.
- Bullock A, Dodington JM, Donoghue AJ, Langhan ML. Capnography Use During Intubation and Cardiopulmonary Resuscitation in the Pediatric Emergency Department. Pediatr Emerg Care. 2017; 33: 457-461.
- Chou HC, Tseng WP, Wang CH, Ma MH, Wang HP, et al. Tracheal rapid ultrasound exam (T.R.U.E.) for confirming endotracheal tube placement during emergency intubation. Resuscitation. 2011; 82: 1279-1284.
- Long B, Koyfman A, Vivirito MA. Capnography in the Emergency Department: A Review of Uses, Waveforms, and Limitations. J Emerg Med. 2017; 53: 829-842.
- Lien WC, Chang CH, Chang WT, Chen WJ. Ultrasonographic Assessment During Cardiopulmonary Resuscitation. J Vis Exp. 2020; 164.