
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Peripheral facial nerve palsy as a presenting symptom of COVID-19 infection: A case report
Narges Karimia1; Athena Sharifi-Razavi2*
1 Associated Professor in Neurology, Toxoplasmosis Research Centre, Immuno genetics Research Centre, Clinical Research Development Unit of Bou-Ali Sina Hospital, Mazandarn University of Medical Science, Sari, Iran.
2 Assistant Professor in Neurology, Clinical Research Development Unit of Bou-Ali Sina Hospital, Mazandarn University of Medical Science, Sari, Iran.
*Corresponding Author : Athena Sharifi-Razavi
Assistant Professor in Neurology, Mazadaran University
of Medical Science, Neurology Department, Bu Ali Sina
Hospital, Pasdaran Boulevard, Sari, Iran.
Email: Athena.sharifi@yahoo.com
Received : Apr 05, 2021
Accepted : May 03, 2021
Published : May 06, 2021
Archived : www.jcimcr.org
Copyright : © Sharifi-Razavi A (2021).
Abstract
New corona virus named as COVID-19 can presented not only by respiratory symptoms, but also with other organs involvement such as gastrointestinal, cardiac, renal and neurological symptoms. We reported a patient who presented with peripheral facial nerve palsy and evaluations revealed COVID-19 infection. We suggest from this case, that COVID-19 infection may be a potential cause of facial paralysis and during this terrible pandemic, neurologists will need to be vigilant for the any neurological manifestation or neurological complications of covid-19.
Citation: Karimia N, Sharifi-Razavi A. Peripheral facial nerve palsy as a presenting symptom of COVID-19 infection: A case report. J Clin Images Med Case Rep. 2021; 2(3): 1116.
Introduction
The pathogen of the now ongoing novel pneumonia pandemic is the severe acute respiratory syndrome coronavirus 2(SARS-CoV-2 or COVID-19). Patients infected with SARS-CoV-2 have symptoms of varying degrees, ranging from fever or a mild cough to pneumonia and extensive involvement of multiple organ functions [1]. New clinical data have reported growing number of COVID-19 patients exhibited only neurological complaint as the initial symptoms such as headache, anosmia, dysgeusia, sensory abnormalities, sphincter disturbances, dizziness, seizure, ischemic stroke, intracerebral hemorrhage, guillain barre syndrome, encephalitis, impaired consciousness and so on [2-6].
Case presentation
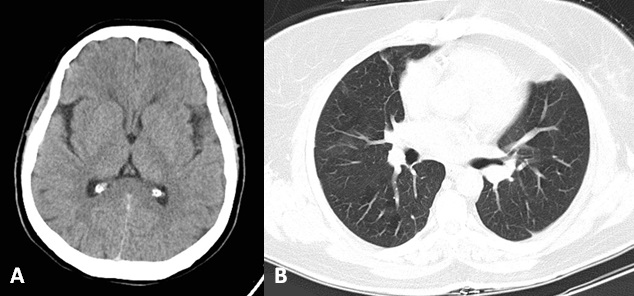
A 53-year-old female referred to outpatient clinic (Tooba clinic, Sari, Iran) with acute right side facial drooping after awakening. She suffered dry cough from 2 months later and mild pain around the right ear from 3 days ago. She had history of diabetes mellitus, hypertension and ischemic heart disease. At visit time, she has no evidence of dyspnea or other respiratory problem. She was afebrile and other vital signs was stable, O2 Sat was 98% on room air. Otoscopy was normal and there was no vesicle on and around the auditory canal. Mild conjunctival congestion in right side was observed. Neurological examination revealed peripheral facial nerve palsy in right side, normal other cranial nerves and other neurological examinations. According to the recent pandemic and complaint of dry cough, Lung CT Scan requested along with brain CT Scan and some laboratory tests. Manuscript File Click here to view linked References laboratory test results indicated WBC: 5700 (Polymorph nuclear: 4332, Lymphocyte 1254 cell per microliter), quantitative CRP: Negative and normal other routine lab tests. Manuscript File Brain CT scan was normal (Figure 1A) and lung CT scan showed mild ground glass opacities in both lungs (Figure 1B). Considering lung CT view, respiratory specimen by nasopharyngeal swab was tested for COVID19 using real-time PCR, that result was positive. Patient treated with tab hydroxychloroquine, azitomycin and acyclovir with favorable recovery after 7 days fallow up visit.
Discussion
Idiopathic peripheral facial nerve paralysis commonly named “Bell's Palsy” is the most cranial neuropathy [10]. The Herpes Simplex Virus (HSV) mediated inflammatory/immune mechanism is widely accepted as the cause of Bell's palsy in most cases [11]. HSV reactivation can lead to inflammation, demyelination, and palsy [12]. Other infectious causes of acute peripheral facial palsy include herpes zoster, cytomegalovirus, Epstein-Barr virus, adenovirus, rubella virus, mumps, influenza B, and coxsackievirus [13]. The peak occurrence of Bell's palsy is usually occurring 1-2 weeks after virus infection, which might be an autoimmune demyelination disease following virus infection [14], suggesting that the palsy is not due to a direct toxic response but rather an induced immune response [15]. Alternate postulated mechanisms of Bell's palsy is ischemia of the facial nerve [16]. Diabetes is a risk factor for microangiopathy, which may lead Bell's palsy via to microcirculatory failure of the vasa nervosum [17]. The exact mechanisms of neurological damage caused by COVID-19 is not yet well known. Some recognized mechanisms is as following: 1) nerve damage through direct infection pathways such as blood circulation and neuronal pathways, 2) hypoxia, 3) immune injury, 4) binding with angiotensin-converting enzyme 2 receptors (ACE2) [18]. Therefore, the potential of facial nerve involvement is not ignorable. So, two hypotheses can be proposed. First, direct invasion of facial nerve through chorda tympani. The chorda tympani is the largest branch of the facial nerve, passes across the tympanic membrane, separated from the middle ear cavity only by a mucous membrane [19] so, can be infected by nasopharyngeal secretions containing virus. In other hand, ACE2 positive cells were widely distributed in the upper respiratory tract, and cells lining salivary gland ducts [20] that innervated by chorda tympani could be source of invasion. The same mechanism has speculated about olfactory nerve involvement [21]. The second hypothesis is effect of immune response and autoimmune demyelination after virus infection similar to other viral causes of Bell’s palsy. Our patient had no acute or active respiratory symptom except dry cough and her lung involvement was not severe. Therefore, there was 2 month durations from the beginning of this symptom. So, It seems the second theory is the speculated mechanism of facial nerve palsy in this patient. Also, it should be considered that our patient was diabetic and microangiopathy could be led to facial nerve paralysis specially during any systemic disorder or infection. In summary, we suggest that COVID-19 infection may be a potential cause of facial paralysis and during this terrible pandemic, neurologists will need to be vigilant for the any neurological manifestation or neurological complications of covid-19.
Authors' contribution: Study concept and design: Athena Sharifi-Razavi. Drafting of the manuscript: Nargeskarimi. Critical revision of the manuscript: Athena Sharifi-Razavi.
Ethical approval: Ethical board committee of Mazandaran University of Medical Sciences approved the publication of this case report.
Funding/support: Mazandaran University of Medical Sciences is source of funding.
References
- Giacomelli A, Pezzati L, Conti F, et al. Self-reported Olfactory and Taste Disorders in Patients With Severe Acute Respiratory Coronavirus 2 Infection: A Cross-sectional Study. Clin Infect Dis. 2020; 71: 889-890.
- Wang HY, Li XL, Yan ZR, et al. Potential neurological symptoms of COVID-19. Therapeutic Advances in Neurological Disorders. 2020.
- Ramezanpour F, Zarvani A, Sharifi-Razavi A. Postpartum Posterior Reversible Encephalopathy Syndrome in Patient Suspected to COVID-9 Infection: A Case Report. Anti-Infective Agent. 2020.
- Fridman S, Bullrich MB, Jimenez-Ruiz A, et al. Stroke Risk, phenotypes, and death in COVID-19: Systematic review and newly reported cases. Neurology. 2020.
- Mardani M, Nadji SA, Sarhangipor KA, et al. COVID-19 infection recurrence presenting with meningoencephalitis. New Microbes New Infect. 2020; 37: 100732.
- Sharifi-Razavi A, Sedaghat Z, Baziboron M, et al. COVID-19 Accompanied with Intracerebral Hemorrhage: A Case Series. Arch Clin Infect Dis. Online ahead of Print; In Press. 2020; e104877.
- Sharifi-Razavi A, Karimi N, Zarvani A, et al. Ischemic stroke associated with novel coronavirus 2019: A report of three cases. International Journal of Neuroscience. 2020; 1-5.
- Liu K, Pan M, Xiao Z, et al. Neurological manifestations of the coronavirus (SARS-CoV-2) pandemic 2019–2020. Journal of Neurology, Neurosurgery & Psychiatry. 2020.
- Sharifi-Razavi A, Karimi N, Rouhani N. COVID-19 and intra cerebral hemorrhage: Causative or coincidental. New Microbes and new infection. 2020.
- Baugh RF, Basura GJ, Ishii LE, et al. Clinical practice guideline: Bell’s palsy. Otolaryngology–Head and Neck Surgery. 2013; 149: S1-S27.
- Bell’s palsy PE. The spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol Suppl. 2002; 4.
- Kennedy PG. Herpes simplex virus type 1 and Bell’s palsy-a current assessment of the controversy. J Neurovirol. 2010; 16: 1.
- Morgan M, Nathwani D. Facial palsy and infection: The unfolding story. Clin Infect Dis. 1992; 14: 263.
- Wan Y, Cao S, Fang Q, et al. Coronavirus disease 2019 complicated with Bell’s palsy: a case report. Research Square. 2020.
- Couch RB. Nasal vaccination, Escherichia coli enterotoxin, and Bell’s palsy. N Engl J Med. 2004; 350: 860.
- Kanoh N, Nomura J, Satomi F. Nocturnal onset and development of Bell’s palsy. Laryngoscope. 2005; 115: 99.
- Riga M, Kefalidis G, Danielides V. The role of diabetes mellitus in the clinical presentation and prognosis of Bell palsy. J Am Board Fam Med. 2012; 25: 819.
- Wu Y, Xu X, Chen Z, et al. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain, Behavior, and Immunity. 2020.
- Monkhouse WS. The anatomy of the facial nerve. Ear Nose Throat J. 1990; 69: 677.
- Liu L, Wei Q, Alvarez X, et al. Epithelial cells lining salivary gland ducts are early target cells of severe acute respiratory syndrome coronavirus infection in the upper respiratory tracts of rhesus macaques. Journal of virology. 2011; 85: 4025–4030.
- Manji H, Carr AS, Brownlee WJ, et al. Neurology in the time of covid19. 2020.