
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
The socket-shield technique and early implant placement for tooth rehabilitation: A case report
Getúlio Batista de Oliveira1; Mariana de Almeida Basilio2; Nara Santos Araujo1; Patricia Ramos Cury3*
1 PhD student, Postgraduate Program in Health and Dentistry, School of Dentistry, Federal University of Bahia, Salvador, Bahia, Brazil.
2 Adjunct Professor, Department of Clinical Odontology, School of Dentistry, Federal University of Bahia, Salvador, Bahia, Brazil.
3 Adjunct Professor, Department of Periodontics, Postgraduate Program in Health and Dentistry, School of Dentistry of the Federal University of Bahia, Salvador, Bahia, Brazil.
*Corresponding Author : Patricia Ramos Cury
School of Dentistry, Federal University of Bahia, Av.
Araújo Pinho, 62, Canela 40110-150, Salvador/Bahia,
Brazil.
Email: patcury@yahoo.com
Received : Apr 03, 2021
Accepted : May 04, 2021
Published : May 07, 2021
Archived : www.jcimcr.org
Copyright : © Cury PR (2021).
Abstract
For a long time, different approaches to minimize the dimensional ridge alteration following tooth extraction have been described even though none of them was capable to avoid alveolar bone loss. The Socket-Shield Technique (SST) seems to be an alternative for alveolar bone preservation in dental extraction planning. This technique conventionally uses a flapless approach and the buccal root portion retention to prevent bone loss. This case report describes the SST with an early implant placement in a patient who presented the nonrestorable tooth # 15 due to the extensive cavity. After six months of the implant placement a porcelain-fused-to-metal crown was fabricated and screwed into the implant with a satisfactory esthetic and functional result. The SST is a non-invasive and effective approach to tooth extraction and rehabilitation, especially in the aesthetic zone. Approximately two-year follow-up shows a satisfactory aesthetic maintenance.
Keywords: Alveolar ridge preservation; Minimally traumatic extraction; Socket shield technique; Tooth extraction.
Citation: Oliveira GBD, Basilio MDA, Araujo NS, Cury PR. The socket-shield technique and early implant placement for tooth rehabilitation: A case report. J Clin Images Med Case Rep. 2021; 2(3): 1118.
Introduction
Soft and hard tissue alteration always happens following tooth extraction. The amount of tissue loss depends on the buccal alveolar bone wall thickness [1], prominent roots [2] and surgical trauma [3-5]. Fifty percent of bone width loss happens in the first year after tooth extraction [6]. Different approaches to minimize the dimensional ridge alteration following tooth extraction have been described [7-10], but they were not capable to avoid bone loss even though high cost techniques have been applied [11,12]. Even an immediate implant may fail to prevent undesirable remodeling bone walls of the tooth socket [13,14].
The root submergence technique maintains the decoronated tooth submerged at or below the alveolar bone level. The maintenance of periodontium ligament yields an alveolar bone nourishing and that is why the bone resorption of this technique is minimal [15]. Based on this concept, Hürzeler et al. [12] developed the Socket-Shield Technique (SST) for alveolar bone preservation with immediate implant placement. They observed that when a tooth portion is retained at the tooth socket the dimensional ridge alteration is minimal. A Proximal Socket Shield (PSS) for interimplant papilla preservation in the aesthetic zone is a technique for bone crest maintenance between the implants [8]. Despite being mostly used with immediate implant placement, Glocker et al. [16] related a case series of SST and implant placement six months later. During re-entry they observed new bone formation in the alveolar bone and residual ridge preserved. Pour et al [17] used a CAD/CAM fabricated surgical guide to facilitate correct implant placement in a socket shield approach. Miltiadis et al [18] published in detail a step-by-step description of the root-membrane technique (another way to nominate SST) and stated that this technique facilitated clinical stability of soft tissue contours during 3 years of follow-up. A retrospective case series of 10 patients treated with the SST showed a low degree of contour changes of the alveolar bone combined with high esthetic outcomes in a five-year follow-up [19]. All those studies reported satisfactory results. However, some emphasized the technique sensitivity [8,16,18,19].
Case report
A 45-year-old woman, with good health status was referred to clinic of the School of Dentistry of the Federal University of Bahia for tooth # 15 rehabilitation. The patient showed a thick gingival biotype, an open bite which she stated that she never desired to treat, and a high smile line (Figure 1a). The clinical examination and the periapical radiograph revealed a non-restorable tooth # 15 (Figure 1b). The residual bone height would not be satisfactory for immediate implant placement. After explaining the risks and benefits of many treatment options, including orthodontic treatment, fixed prosthesis and removable partial denture, the patient consented to the SST and an implant-supported restoration. A consentment term was then signed by the patient.

Before initiating the surgical procedures, the patient rinsed her mouth with 0.12% chlorhexidine gluconate. A local anesthetic (2% mepivacain with epinephrine 1:100.000, DFL) was injected into the mucosa buccally and palatally. The provisional cement was removed with a spherical diamond bur (1012, KG Sorensen) and, in the buccal side, the coronal root portion was worn with a wheel diamond bur (3053, KG Sorensen) to the bone level. Under abundant saline cooling the root was sectioned in the mesial-distal direction with a long flame diamond bur (3195, KG Sorensen) (Figure 2a). After that, with the same bur, the root buccal portion was cut into a concave shape. The root palatine portion was carefully luxated using of a modified lever form through and making gentle movements (Figure 2b). Then, it was removed with root forceps. The picture shows the root palatine portion (Figure 2c).
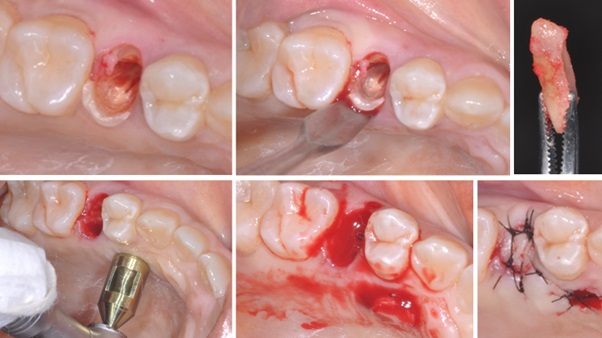
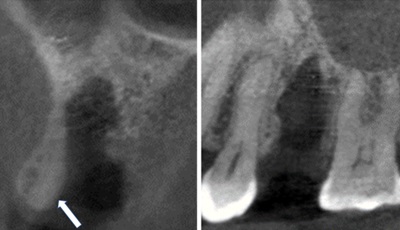
After administration of local anesthesia, a 6 mm diameter circular free gingival graft was removed from the palatal region with circular scalpel (hospital and dental instruments, maximus, Brasil) (Figure 2d). The epithelial tissue was removed from the gingival sulcus with a wheel diamond bur (3053, KG Sorensen) and the dental extraction alveolus was filled with blood collected from the graft donor area (Figure 2e). The donor area was carefully sutured with several x-shaped stitches (nylon 4.0 strand, ethicon) and the gingival graft was sutured on the alveolar wound with single stitches (nylon 5.0 strand, ethicon) (Figure 2f). The coronal cut tomography image shows the shield linked to the buccal alveolar bone (Figure 3a). The sagittal cut tomography image shows the proximity of the tooth alveolus bottom with maxillary sinus (Figure 3b).
Two grams of amoxicillin (EMS Sigma Pharma LTDA, Brazil) and 8 milligrams of dexamethasone (EMS Sigma Pharma LTDA, Brazil) were used 30 minutes before the surgery and 500 milligrams of dipyrone (Medley Industria Farmaceutica Ltda, Brazil) every 6 hours for 48 hours. The patient was instructed not to brush at the surgical area but to rinse with 0.12% chlorhexidine gluconate twice a day (A Formula - Farmácia De Manipulacão, Brasil) for two weeks. After one week, the patient returned to remove the suture from the donor area and after two weeks the suture from the gingival graft was removed.
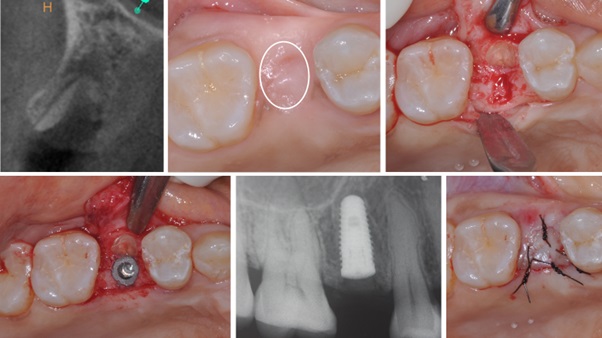
One hundred days following the SST, the coronal cut tomography image showed a socket healing and the root buccal portion (Figure 4a). The healing process occurred uneventfully and ridge width was maintained (Figure 4b). The same medication protocol for the SST surgery was applied for implant placement. A palatalized incision was made on the alveolar ridge mucosa and a partial thickness flap was elevated. The width of the preserved alveolar ridge could be seen with the presence of the root buccal portion attached to the buccal alveolar wall (Figure 4c). After implant bed preparation, a conic morse cone dental implant (3.75x10.0, PROS) was installed in correct three-dimensional position close to the shield without touching it (Figure 4d). The periapical radiograph showed the positioning of the implant (Figure 4e). The surgical wound was carefully sutured with single stitches (nylon 5.0 strand, ethicon) (Figure 4f).
After four months implant installation, the re-opening was performed with the circular scalpel (“Punch” 5,1 mm – ICE) and a healing cap was installed and kept for 7 days. Prior to molding, a provisional healer was made with the healing cap and self-curing acrylic (alike, GC) that was screwed over implant and remained for 7 days for conditioning the gum (Figure 5a). The alveolar ridge volume was preserved and the conditioned gum was observed (Figure 5b). The dental impression was performed by using addition silicone (express, 3M) and the casts were made in type IV gypsum (durone, Dentsply). The PFM crown was made of nickel-chromium metal (High Bond) and feldspathic porcelain (Noritake). The crown was screwed directly to implant, the screw pass hole was filled with composite resin (Filtek® P60 3M ESPE) and the occlusal contact adjustment was done. The harmony of the PFM crown with the neighboring teeth was achieved (Figure 5c). The periapical radiograph showed the satisfactory fitting of the PFM crown (Figure 5d). After 30 days of crown installation, the patient returned to the reassessment. She was very satisfied with the final results and the clinic exam showed a healthy soft tissue around the tooth crown (Figure 5e). Six months later, the patient returned for an evaluation scheduling and the soft tissue around the tooth crown was in a healthy and stable condition (Figure 5f).

Discussion
The patient's aesthetic demand combined with the proximity of the root apex with the maxillary sinus, indicated that the good treatment option for this case was an early implant placement. This case report showed that retaining a well-defined concave shaped root buccal fragment into to the tooth socket resulted in an alveolar ridge preservation. In addition, it was possible to install an early dental implant in the ideal position without difficulties. In the present case, no graft material was used to alveolar preservation but only the shield and clotted blood to fulfill the tooth socket and a soft tissue graft harvested from the palate to coverage the wound. The SST overcomes the high cost of biomaterials used in the guided bone regeneration techniques. Contrary, most alveolar preservation techniques apply expensive materials and invasive approaches [11,16-19].
Many authors have advised the high sensitivity of this technique and therefore should not be recommended as a routine dental practice [8,16-18,20]. The author of this clinical case has made an extensive training on pig’s jaws before performing the surgeries in patients.
Conclusion
This case report showed an alveolar bone preservation approach in an esthetic demand area. The SST demonstrated the maintenance of contour tissue that facilitate three-dimensional implant positioning. The low cost of this technique with good esthetic result and the maintenance of the healthy tissue contour surrounding the metal-ceramic crown encourage the dentists to indicate this technique. Nevertheless, further studies with long-term follow-up are necessary to consolidated this technique. Besides that, good training on animal model is necessary before performing this technique in human beings.
References
- Araújo MG, Wennström J, Lindhe J. Modeling of the buccal and lingual bone walls of fresh extraction sites following implant installation. Clin Oral Impl Res. 2006; 17: 606–614.
- Nevins M, Camelo M, De Paoli S, Friedland B, Schenk RK, et al. A study of the fate of the buccal wall of extraction sockets of teeth with prominent roots. Int J Periodontics Restorative Dent. 2006; 26: 19-29.
- Chu SJ, Salama MA, Garber DA, Salama H, Sarnachiaro GO, et al. Flapless Postextraction Socket Implant Placement, Part 2: The Effects of Bone Grafting and Provisional Restoration on Periimplant Soft Tissue Height and Thickness-A Retrospective Study. Int J Periodontics Restorative Dent. 2015; 35: 803–809.
- Engelke W, Beltrán V, Decco O, Valdivia-Gandur I, Navarro P. Changes in morphology of aveolar buccal walls following atraumatic internal root fragmentation. Int J Morphol. 2015; 33: 491- 496.
- Fickl S, Zuhr O, Watchel H, Bolz W, Hürzeler M. Tissue alterations after tooth extraction with and without surgical trauma: A volumetric study in the beagle dog. J Clin Periodontol. 2008; 35: 356-363.
- Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone Healing and Soft Tissue Contour Changes Following Single Tooth Extraction: A Clinical and Radiographic 12-Month Prospective Study. Int J Periodontics Restorative Dent. 2003; 23: 313–323.
- Araújo MG, da Silva JC, de Mendonca AF, Lindhe J. Ridge alterations following grafting of fresh extraction sockets in man. A randomized clinical trial. Clin Oral Implants Res. 2015; 26: 407–412.
- Kan JY and Rungcharassaeng K. Proximal socket shield for interimplant papilla preservation in the esthetic zone. Int J Periodontics and Restorative Den. 2013; 33: 24-31.
- Kotsaki G, Chrepa V, Marcou N, Prasad H, Hinrichs J. Flapless Alveolar Ridge Preservation Utilizing the Socket-Plug’ Technique: Clinical Technique and Review of the Literature. J Oral Implantol. 2014; 40: 690-698.
- Chen ST, Buser D. Esthetic Outcomes Following Immediate and Early Implant Placement in the Anterior Maxilla, A Systematic Review. Int J Oral Maxillofac Implants. 2014; 29: 186-215.
- Barakat, DA, Hassan RS, Riham M, Eldibany RM. Evaluation of the socket-shield technique for immediate implantation. Alexandria Dent J. 2017; 42: 155-161.
- Hürzeler MB, Zuhr O, Schupbach P, Rebele SF, Emmanouilidis N, et al. The socket-shield technique: A proof-of-principle report. J Clin Periodontol. 2010; 37: 855-862.
- Abadzhiev M, Nenkov P, Velcheva P. Conventional immediate implant placement and immediate placement with socketshield technique – Which is better. Int J Clin Med Res. 2014; 1: 176-180.
- Chappuis V, Araujo MG, Buser D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontol 2000. 2017; 73: 73–83.
- Salama M, Ishikawa T, Salama H, Funato A, Garber D. Advantages of the root submergence technique for pontic site development in esthetic implant therapy. Int J Periodontics Restorative Dent. 2007; 27: 521–527.
- Glocker M, Attin T, Schmidlin PR. Ridge Preservation with Modified “Socket-Shield” Technique: A Methodological Case Series. Dent J. 2014; 2: 11-21.
- Pour RS, Zuhr O, Hürzeler MB, Prandtner O, Rafael CR, et al. Clinical Benefits of the Immediate Implant Socket Shield Technique. J Esthet Restor Dent. 2017; 29: 93-101.
- Mitsias ME, Siormpas KD, Kontsiotou-Siormpa E, Garber D. A step-by-step description of PDL-mediated ridge preservation for immediate implant rehabilitation in the esthetic region. Int J Periodontics Restorative Dent. 2015; 35: 835-841.
- Bäumer D, Zuhr O, Rebele S, Hürzeler M. Socket shield technique for immediate implant placement—Clinical, radiographic and volumetric data after 5 years. Clin Oral Implants Res 2017; 28: 1450–1458.
- Gluckman H, Du Toit J, Salama M, Nagy K, Dard M. A decade of the socket-shield technique: A step-by-step partial extraction therapy protocol. Int J Esthet Dent. 2020; 15: 212-225.