
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
TTE guided synchronization to optimize AV synchronous leadless pacemaker programming
George Mawardi1*; Patricia Rodriguez1; Sula Mazimba1; Nishaki Mehta1,2
1 Department of Cardiovascular Medicine, University of Virginia, 1215 Lee St, Charlottesville, VA 22908, USA.
2 William Beaumont Oakland University of Medicine, Royal Oak, MI 48009, USA
*Corresponding Author : George Mawardi
Department of Cardiovascular Medicine, University
of Virginia, 1215 Lee St, Charlottesville, VA 22908,
USA.
Email: Gm7xd@virginia.edu
Received : Apr 07, 2021
Accepted : May 04, 2021
Published : May 07, 2021
Archived : www.jcimcr.org
Copyright : © Mawardi G (2021).
Citation: Mawardi G, Rodriguez P, Mazimba S, Mehta N. TTE guided synchronization to optimize AV synchronous leadless pacemaker programming. J Clin Images Med Case Rep. 2021; 2(3): 1120.
Introduction
Transvenous pacemakers are associated with major complications [1]. Transcatheter leadless pacemaker has reduced the incidence of these complications and the recent accelerometer based atrial sensing algorithm permits restoration of atrioventricular synchrony [1]. We report utilizing cardiac output measurements using Transthoracic Echocardiography (TTE) to determine optimal programming for leadless pacemaker.
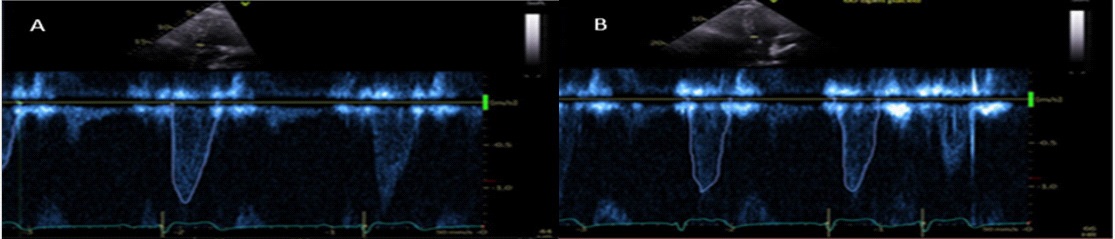
A 69-year-old Caucasian male with a past medical history significant for schizoaffective disorder was admitted to the intensive care unit with acute encephalopathy secondary to a urinary tract infection and superficial skin infection. He responded to tailored antibiotic therapy with fluid management. He was noted to have prolonged sinus pauses and complete heart block and underwent semi-permanent pacemaker implantation after exonerating reversible causes. Two of his antipsychotic medications (olanzapine and lithium) were held with improvement of sinus node function. However, he would require these medications for management of his schizoaffective disorder, and thus underwent uneventful Atrio-Ventricular (AV) synchronous leadless pacemaker implantation. His baseline HR were in the 50s and although he had tolerated asynchronous pacing with his semi-permanent device, optimal cardiac outputs with bedside TTE were compared with VVI 60 and VDD 40 to permit tracking of sinus bradycardia (Figure 1 & Table 1). With similar cardiac outputs, final programming was established at VDD 40.
Single-chamber pacemakers are used in those who do not require frequent pacing, or have vascular access issues or certain comorbidities. However, these devices do not provide the benefit of AV synchrony [2]. Further, several patients with complete heart block may have concomitant sinus node dysfunction [3]. Therefore, the programming algorithm at a higher pacing rate would lead to loss of AV sensing. Our patient represents this clinical dilemma. We utilized echocardiography to determine cardiac output as above. This simple maneuver improved our bedside decision making in that in the setting of sinus note dysfunction, tracking the sinus rate albeit slower, had more favorable hemodynamic effects with transthoracic thoracic guided programming.
Table 1: Cardiac Outputs (CO) of the Left Ventricle (LV) and Right Ventricle (RV), with VVI and Atrio-Ventricular (AV) synchrony.
|
VVI-60 |
AV- VDD40 |
LV CO |
7.4 L |
6.2 L |
RV CO |
6.5 L |
5.6 L |
Acknowledgments: The authors of this study would like to thank the University of Virginia transthoracic echocardiography technologists and Medtronic representatives for their help in this study
References
- Steinwender C, Khelae SK, Garweg C, et al. Atrioventricular Synchronous Pacing Using a Leadless Ventricular Pacemaker: Results From the MARVEL 2 Study. JACC: Clinical Electrophysiology. 2020; 6: 94-106.
- Chinitz L, Ritter P, Khelae SK, et al. Accelerometer-based atrioventricular synchronous pacing with a ventricular leadless pacemaker: Results from the Micra atrioventricular feasibility studies. Heart Rhythm. 2018; 15: 1363-1371.
- Swiatecha G, Sielski S, Wilczek R, et al. Atrioventricular Conduction Disturbances in Patients with Sinoatrial Node Disease and Atrial Pacing. Pacing Clin Electrophysiol. 1992; 15: 2074-2076.