
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Pontine and extra-pontine osmotic demyelination syndrome: Case report
Eduardo dos Santos Sousa*; Felipe Teijeiro Cabral; Annelise Akemi Higa Lee; Francisco Tomaz Meneses de Oliveira; Rubens José Gagliardi
Department of Neurology, Rua Dr. Cesário Mota Jr, 112, Ed. Conde de Lara, 3rd floor, Vila Buarque, Sà £ o Paulo-SP, Brazil.
*Corresponding Author : Eduardo dos Santos Sousa
Department of Neurology, Rua Dr. Cesário Mota Jr,
112, Ed. Conde de Lara, 3rd floor, Vila Buarque, SÃ £ o
Paulo-SP, Brazil.
Email: eduardosousa.neuro@gmail.com
Received : Apr 07, 2021
Accepted : May 04, 2021
Published : May 07, 2021
Archived : www.jcimcr.org
Copyright : © Sousa EDS (2021).
Abstract
Osmotic demyelination syndrome is a rare disease, clinically presented as a global reduction in strength, tetraparesis, variations in the level of consciousness, and its content, and comatose status, associated with rapid variances in serum sodium levels (whether hyponatremia or hypernatremia). The neuroimaging findings are mainly in the pontine region, but currently the number of reports of extrapontine involvement has increased, typically with lesions in the topography of the thalamus, cerebellum, midbrain (substantia nigra), corpus callosum and hypothalamus. We display a rare case of pontine and extra-pontine involvement, even after the sodium replacement protocols of the current guidelines.
Keywords: Hyponatremia; Osmotic demyelination; Myelinolysis; Pontine; Extra-pontine.
Citation: Sousa EDS, Cabral FT, Lee AAH, Oliveira FTMD, Gagliardi RJ. Pontine and extra-pontine osmotic demyelination syndrome: Case report. J Clin Images Med Case Rep. 2021; 2(3): 1121.
Introduction
Osmotic demyelination syndrome is a rare disease, with unknown prevalence, but it is widely recognized as an entity with high morbidity and mortality and an equivalent prevalence in both sexes [1].
The clinical presentation is usually associated associated with rapid variances in serum sodium levels, whether hyponatremia or hypernatremia. Originally the neuroimaging findings are mainly in the pontine region, but currently the number of re � - ports with extra-pontine involvement has increased, typically with lesions in the topography of the thalamus, cerebellum, midbrain (substantia nigra), corpus callosum and hypothalamus [3].
Clinically presented as a global reduction in strength, tetraparesis, variations in the level of consciousness, and its content, and comatous status [4-6]. Symptom onset usually occurs 2 to 7 days after osmolarity variation [3].
Magnetic Resonance Imaging (MRI) of the skull can show lesions that are generally symmetrical, hypointense in T1-weighted sequences and hyperintense in T2 and FLAIR, developing after the first week of clinical presentation, highlighting the importance of continuing to investigate the neuroimaging even in if it suggests normal findings in the first presentation [3,7]. Histopathological findings reveals lesions of the myelin sheaths with preservation of the axons and nerves of the pontine nucleus, without the association of an inflammatory component, which distinguishes these cases from diseases such as Multiple Sclerosis, Neuromyelitis Optica and ADEM, among other inflammatory diseases of the central nervous system [6-8].
Currently, there is still no specific treatment established, but the identification of patients at risk is the first step to provide adequate support.
Case report
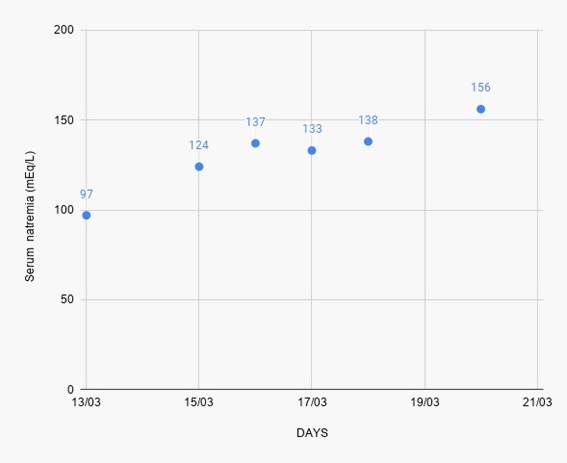
Female patient, 66 years old, from São Paulo-SP, with a history of Acute Myocardial Infarction and Essential Thrombocythemia on regular use of hydroxyurea (500 mg/day) chlortalidone (25 mg/day), acetylsalicylic acid (100 mg/day) , desvenlafaxine (100 mg/day), and recent use of lithium, oxcarbazepine and quetiapine due to depressive symptoms. She had been admitted to the emergency department with nausea and vomiting; three days after admission, she progressed rapidly with lowering of consciousness, bradypsychism, hyporexia. In admission exams, severe hyponatremia was found (serum Na: 97 mEq/L). Intravenous sodium replacement was started, following the sodium correction guidelines, aiming not to exceed more than 8-10 mEq/day, but even with all caution to sodium replacement, the patient develops a rapid increase in serum sodium levels (Figure 1).
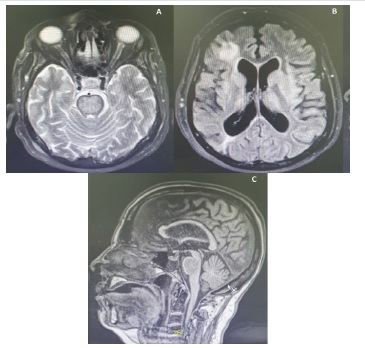
Due to the persistence of coma and tetraparesis with signs of pyramidal release, the investigation was carried on with a MRI of the skull (Figure 2), which showed hypersignal in the central region of the bridge from the level of the lower cerebellar peduncles to the mid-mesencephalic transition sparing the corticospinal tracts. Bilateral base nucleus hypersignal and small foci of cortico-subcortical hypersignal with a pontine and extra-pontine demyelination pattern also becaming evident. The patient progresses with acute respiratory failure of probable infectious etiology and she is then intubated and admitted to the intensive care unit. She remained in an non-perceptive and non-reactive coma despite the removal of sedation.
Discussion
The osmotic demyelination syndrome is characterized by a condition that can lead to different neurological deficits [10]. Pathophysiology possibly involves an injury to the neuronal sheath resulting from the rapid modification of the osmotic flow in the oligodendrocyte, the cell most affected in these cases. During the correction of hyponatremia, if the rate of increase in tonicity is faster than the rate of formation and / or transport of organic substractes to cells, it will tend to dehydration, resulting in apoptosis [9].
In this case, the patient was admitted with severe hyponatremia and evolved with a natremia increase of 36mEq / L in 24 hours. When the complementary neuroimaging exam was performed, it showed lesions in pontine topography with osmotic demyelination characteristics, which combined to the clinical-laboratory context, allowed the diagnosis of pontine and extra-pontine myelinolysis. The underlying cause of hyponatremia is still being investigated, but we believe that it is probably drug-based, multifactorial, and the hypothesis of intoxication by antidepressant, thiazide, neuroleptic and lithium drugs is suggested. The investigation was widened to disorders of the hypothalamic-pituitary axis, adrenal and thyroid disorders, in addition to tubular nephropathies [2].
The prognosis of the disease is reserved in a large proportion of the cases, with description of high mortality related to complications due to the length of hospital stay, immobilization syndrome and frailty syndrome [11], there are also reports of total recovery without neurological sequelae [10]. It is also known that no current treatment has been proved effective in reversing the condition, thus, the patient in question received all clinical and assistance support, as well as the necessary clarifications to the family members.
Conclusion
The importance of presenting this case lies not only in the fact that it is an uncommon pathology, which must be presented to all clinical doctors and specialists, but mainly to alert doctors who work on emergency rooms of the importance and caution of sodium replacement, even in smaller volumes than its recommendation in the current literature, as the sequelae can be much greater than hyponatremia itself. Also we must always look for the incessant investigation of the underlying cause of hyponatremia, as well as the importance of repeating neuroimaging in some cases after the first week of investigation.
References
- Bento S, Augusto A, Jacinto Lj. Mielinólise pontina: A propósito de um caso clínico. Revista as Sociedade Portuguesa de Medicina Física e de Reabilitação. 2013; 23.
- Adams RD, Victor M, Mancall EL. Central pontine myelinolysis: a hitherto undescribed disease occurring in alcoholic and malnourished patients. AMA Arch Neurol Psychiatry. 1959; 81: 154- 172.
- Osborn AG, Hedlund GL, Blaser SI, Illner A, Salzman KL, et al. Osmotic demyelination syndrome. In: Diagnostic imaging brain. Salt Lake City: Amirsys. 2004; 10: 42-45.
- Victor M, Ropper AH. The acquired metabolic disorders of the nervous system: central pontine myelinolysis. In: Victor M, Ropper AH. Adams and Victor’s principles of neurology. 7th ed. New York: McGraw-Hill. 2001: 1193-1195.
- Martin RJ. Central pontine and extra-pontine myelinolysis: the osmotic demyelination syndromes. J Neurol Neurosurg Psychiatry. 2004; 75: 22-28.
- Brown WD, Caruso JM. Extrapontine myelinolysis with involvement of the hippocampus in three children with severe hypernatremia. J Child Neurol. 1999; 14: 428-433.
- Laureno R, Karp BI. Myelinolysis after correction of hyponatremia. Ann Intern Med. 1997; 126: 57-62.
- Haspolat S, Duman O, Senol U, Yegin O. Extrapontine myelinolysis in infancy: Report of a case. J Child Neurol. 2004; 19: 913- 915.
- Ruzeka KA, Campeaua NG, Miller GM. Early diagnosis of central pontine myelinolysis with Diffusion-Weighted Imaging. American Journal of Neuroradiology. 2004; 25: 210-213.
- Brito AR, Vasconcelos MM, Júnior LCHE, et al. Central Pontine and extrapontine myelinolysis: Report of a case with a tragic outcome. Jornal de Pediatria. 2006; 82: 157-160.
- Ashrafian H, Davey P. A review of the causes of central pontine myelinosis: Yet another apoptotic illness?. European Journal Neurology. 2001; 8: 103-109.