
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Management of progressive spine deformity in a child with pseudoachondroplasia
Sergey Ryabykh1; Polina Ochirova2; Alexander Gubin2; Alexander Burtsev1; Marat Saifutdinov1; Ali Al Kaissi1
1National Medical Research Center for Traumatology and Ortopedics n.a. G.A. Ilizarov, Kurgan, Russia.
2 National Medical Research Center of Traumatology and Orthopedics n.a. N.N. Priorov, Moscow, Russia.
*Corresponding Author : Ali Al Kaissi
National Medical Research Center, Ilizarov, Kurgan,
Russia.
Email: kaissi707@gmail.com
Received : Apr 08, 2021
Accepted : May 04, 2021
Published : May 07, 2021
Archived : www.jcimcr.org
Copyright : © Kaissi AA (2021).
Abstract
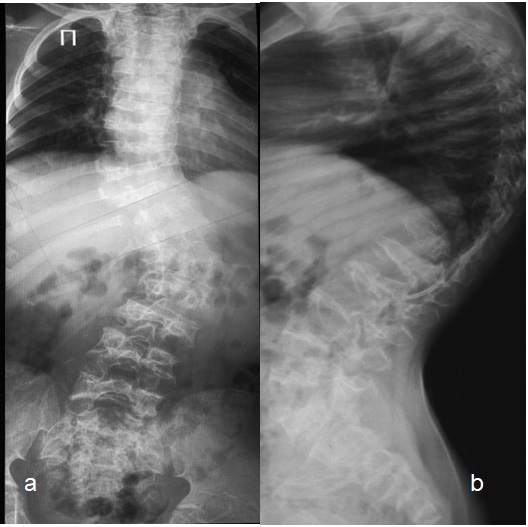
Short-limbed dwarfism, knock knees and joint hypermobility are the classical clinical criteria encountered in patients with pseudoachondroplasia. Progressive kyphoscoliosis was the main clinical presentation in our patients with pseudoachondroplasia. Preoperative spine radiographs in an 13-years-old-girl showed severe kyphoscoliotic deformity (kyphosis - 70o and scoliosis of Cobbs angle – 55o ).
Keywords: Pseudoachondroplasia; COMP gene mutation.
Citation: Kaissi AA, Ryabykh S, Ochirova P, Gubin A, Burtsev A. Management of progressive spine deformity in a child with pseudoachondroplasia. J Clin Images Med Case Rep. 2021; 2(3): 1123.
Introduction
Maroteaux and Lamy described a syndrome of short stature previously confused with achondroplasia or in some instances with Morquio´s syndrome [1]. Pseudoachondroplasia is characterised by short-limbed dwarfism in which both the epiphyses and metaphyses are involved. Affected individuals have significantly short stature, loose ligaments and a predisposition to premature Osteoarthritis (OA). Pseudoachondroplasia is usually transmitted as an autosomal dominant traithe joints most commonly affected are the large weight-bearing joints of the lower limbs. Classically, the radiographs reveal fragmented epiphyseal ossification centers of the long bones with mild involvement of the vertebrae [1-3]. Baily [4] considered pseudoachondroplasia as the most common condition of dwarfism encountered in orthopaedic surgery. Congenital kyphoscoliosis results from developmental vertebral anomalies that interferes adversely with the normal longitudinal growth anterior or anterolateral to the transverse axis of vertebral rotation in the sagittal plane [5].
Case presentation
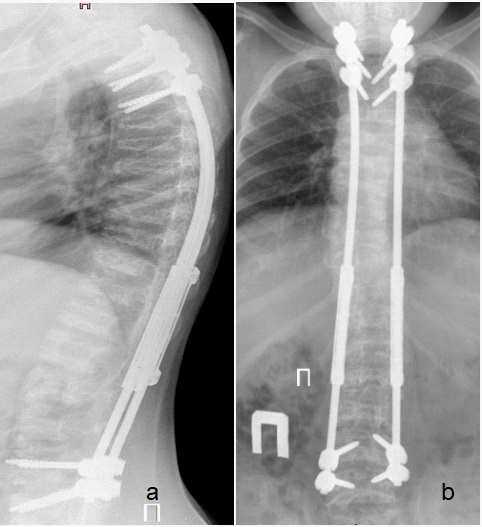
A 13-years-old-girl presented with the phenotype/genotype of pseudoachondroplasia. She was referred to our department because of progressive thoracolumbar kyphoscoliosis. Anteroposterior spine radiographs showed scoliosis of 55° Cobb’s angle (Figure 1a). Lateral spine radiograph showed appearance of anterior ring epiphysis indentations with severe platyspondyly and kyphosis of 70° Cobb’s angle (Figure 1b). She manifested standing height before finalization of growing rod intervention of 146 cm, her forced vital capacity was around 60-70% and her forced expiratory volume in the first second was around 85-90% of expected. For her kyphoscoliosis deformity she underwent «Growing Rod» construction. The latter was followed by final intervention to rectify her kyphoscoliotic deformity after five years follow-up, this has been performed via final posterior fusion Th2-L5 (Posterior spondilodesis). Posteoperative spine radiographs showed scoliosis minimized to 5° Cobbs angle and kyphosis to 50°) (Figure 2a,b).
Discussion
Radiographs in pseudo achondroplasia revealed biconvex vertebral bodies in infancy, with an anterior tongue later on. In adult life the vertebrae can show platyspondyly, or be of normal height, but they have the normal rectangular shape. Long pedicles, irregular upper and lower sufaces and odontoid hypoplasia may be noted.
In practice, studies described the usage of growing rods for curves exceeds 60° for patients of less than 10 years-old, showed no fixed agreement regarding the perfect age of surgical interventions and or any other procedures taken [7]. Literature review showed that the vast majority of patients underwent growing surgery were mostly over the age of 10 years. Effective intervention is around five years, in which patients are eligible to undergo several procedures within this period.
Elsebai et al., collected and analyzed the data of 19 patients with congenital deformities. All underwent growing rod treatment. Correction of the deformities and preservation of growth resulted during intervention were found to be persuasive in comparison to the results achieved in patients with with idiopathic-type. They observed dramatic improvements in space available for the lung ratio which offers better space for lung functions. They confirmed the safety and the efficacy of the growing rods in patients with developmental spine deformities [8].
Growing rod treatment has been applied successfully to patients with other types of connective tissue disorders such as Marfan syndrome. Skaggs et al. [9] studied 10 patients with spine deformities manifested itself before the age of 3-years. These children were treated via the application of growing rod technique and lengthening which was performed once a year for patient’s under-anti-coagulant therapy. 60% mean curve correction for dual rods have been achieved, associated with overall length of 11.5 cm. Complications have been recorded to include two rod breakages, one anchor dislodgement, and three intraoperative dural leaks. The authors concluded that growing rods are an effective treatment for early-onset deformity in Marfan syndrome, helping prevent large infantile curves from becoming severe and allowing definitive fusion closer to skeletal maturity. Acute heart failure following growing rod surgery for Marfan syndrome-related scoliosis has been described, mostly resulted from mechanical torsion of the cardio-vasculature due to over-distraction. Reversing of the symptoms were noticed after release of the distraction.
Conclusion
Some children with pseudoachondroplasia might manifest spine deformities at any age. The onset of appearance of spine deformities in this group of patients differs and ranging between early-childhood-onset spine deformities to pre-adolescent onset type. Regardless the age of onset, an eye should be kept to assess and control articular and axial deformities through clear strategy. The purpose is to ensure the fulfillment of better skeletal maturity.
References
- Maroteaux P, Lamy. Pseudo-achondroplastic forms of spondyloepiphyseal dysplasias. Presse Med. 1959; 25; 67: 383–386.
- Maroteaux P, Stanescu R, Stanescu V, et al. The mild form of pseudoachondroplasia. Eur J Pediatr. 1980; 133: 227-231.
- Al Kaissi A, Ghachem MB, Kenis V, Melchenko E, Grill F, Ganger R, Kircher SG. A constellation of orthopaedic deformities in connection with cartilage oligomeric matrix protein mutation. Afr J Paediatr Surg. 2019; 16: 23-28.
- Al Kaissi A, Zandieh S, Haller J, Klaushofer K, Grill F. Dolichoodontoid in a boy with pseudoachondroplasia. European Journal of Orthopaedic Surgery & Traumatology. 2008; 18; 297-301.
- Bailey JA. Disproportionate short stature. WB Saunders, London. 1973.
- McMaster MJ, Singh H. Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am. 1999; 81: 1367–1383.
- Mahar AT, Bagheri R, Oka R, Kostial P, Akbarnia BA. Biomechanical comparison of different anchors (foundations) for the pediatric dual growing rod technique. Spine J. 2008; 8: 933–939.
- Elsebai HB, Yazici M, Thompson GH, et al. Safety and efficacy of growing rod technique for pediatric congenital spinal deformities. J Pediatr Orthop. 2011; 31: 1–5.
- Skaggs DL, Bushman G, Grunander T, Wong PC, Sankar WN, et al. Shortening of growing-rod spinal instrumentation reverses cardiac failure in child with Marfan syndrome and scoliosis. A case report. J Bone Joint Surg Am. 2008; 90: 2745–2750.