
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A rare complication of STEMI: Anaphylactic shock post-fibrinolytic
Teddy Arnold Sihite1,2*; Muhammad Hafizh Dewantara1; Mega Febrianora2
1Department of Internal, Hasan Sadikin General Hospital, Universitas Padjadjaran, Bandung, Indonesia.
2 Department of Cardiology and Vascular Medicine, Hasan Sadikin General Hospital, Universitas Padjadjaran, Bandung, Indonesia.
*Corresponding Author : Teddy Arnold Sihite
Department of Internal Medicine, Hasan Sadikin General Hospital, Jalan Eyckman 38, Bandung 40161, Indonesia.
Email: teddysyhyte@yahoo.com
Received : Apr 09, 2021
Accepted : May 04, 2021
Published : May 07, 2021
Archived : www.jcimcr.org
Copyright : © Sihite TA (2021).
Abstract
ST-Elevation Myocardial Infarct (STEMI) is the most common emergency condition that causes sudden death. The revascularization speed of the occluded coronary artery is the key to success in STEMI management in both aspects of reducing morbidity and mortality. Primary Percutaneous Coronary Intervention (PCI) is the first line of reperfusion management in the treatment of STEMI patients, but in some conditions, such actions cannot be performed then pharmaco-invasive strategies should be done. There are several complications of STEMI after fibrinolytic therapy. In this case report, we presented a rare complication of anaphylactic shock in STEMI patient underwent fibrinolytic therapy.
Keywords: Anaphylactic shock; Fibrinolytic; PCI; STEMI.
Citation: Sihite TA, Dewantara MH, Febrianora M. A rare complication of STEMI: Anaphylactic shock post-fibrinolytic. J Clin Images Med Case Rep. 2021; 2(3): 1127.
Introduction
STEMI occurs due to an atherosclerotic process in the coronary arteries that can cause an imbalance condition between oxygen demand and supply on the myocardial. If the reperfusion is not performed immediately, it will cause irreversible myocardial necrosis. The first-line management for STEMI patients is primary PCI, however, in some conditions, such action cannot be performed so pharmaco-invasive strategies, such as fibrinolytic, need to be performed [1].
Streptokinase is a fibrinolytic agent that is widely used in developing countries because it is more economical than the latest generation of fibrinolytic, such as tissue plasminogen activator (tPA) [2]. Fibrinolytic agents in addition to causing bleeding, can also cause allergic reactions. Streptokinase has been reported to be antigenic, it is activating antibodies in individuals who have obtained the agent for the first time causing severe type I hypersensitivity reactions such as anaphylactic shock [3]. The following will be discussed a case reports on consideration of the selection of reperfusion management for STEMI patients.
Case illustration
Male 67 years-old came with chest pain as his chief complaint. The patient said it happened when he was on a rest 8 hours before admission. The chest pain was radiating to his back for about 30 minutes and happens constantly. Complaints were accompanied by cold sweats that make his body wet without nausea or vomiting. The patient did not complain bout shortness of breath, palpitation, fainting, or almost fainting. When the patient just arrived at the hospital, the chest pain still felt.
The patient had a history of shortness of breath during severe activity that getting better with rest since 3 months ago. The patient also had a history of chest pain during severe activity since 1 month ago. The patient has had hypertension for the last 10 years. The patient was an active smoker since young. There is no history of Diabetes Mellitus, dyslipidemia, or family history of the acute coronary syndrome.
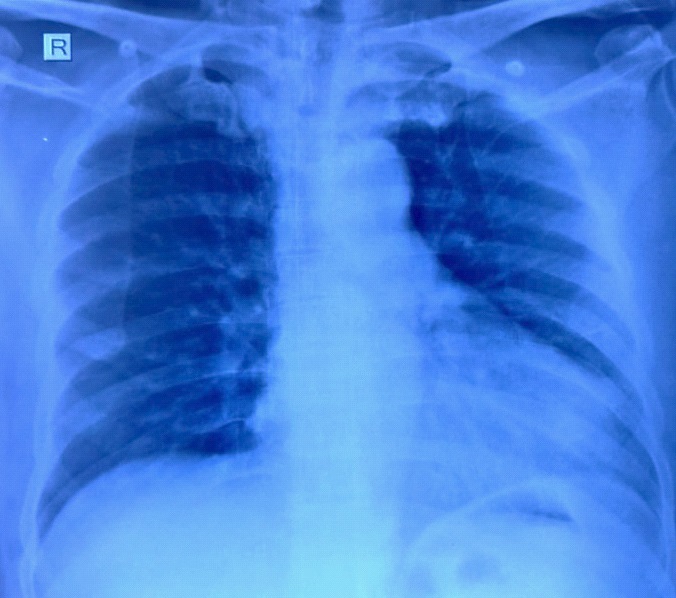
On the physical examination, general condition was mildly ill, compos mentis, blood pressure 150/90 mmHg, pulse 52x/minute, respiration 20x/minute, temperature 36,8oC, oxygen saturation 97% with free air. From head and neck examination, the jugular vein is 5+2 cm H2O. From heart examination, there is left heart enlargement without additional heart sound or murmur. From the lung examination, there is no sign of ronchi or wheezing. Other examinations were within the normal limit.
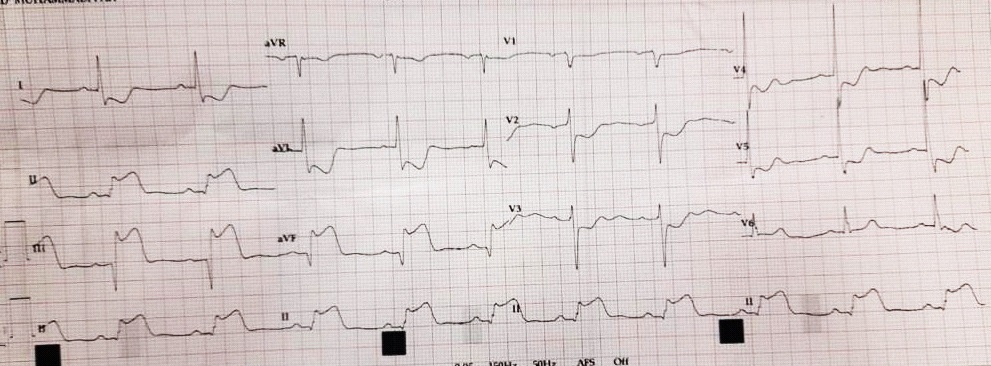
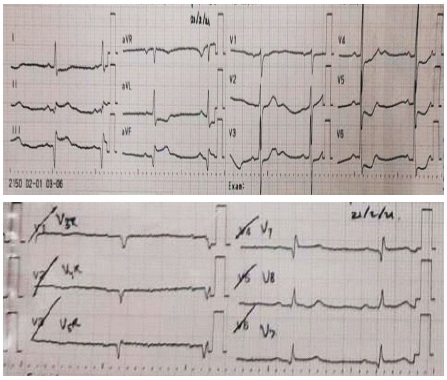
The laboratory examination showed slightly leukocytosis 11230 /uL. The chest X-ray revealed cardiomegaly. Two hours after onset, the hospital showed sinus rhythm, STEMI inferior wall, anterolateral-high lateral ischemic dd/ reciprocal. Electrocardiography at eight hours after onset showed sinus bradycardia, infero-posterior wall STEMI with evolution. According to pandemic protocol, the patient had a COVID-19 test and the PCR result was negative.
This patient was then diagnosed with ST-elevation Myocardial Infarction. The patient already got aspirin loading dose 162 mg and Clopidogrel 1X300 mg from the previous hospital. Other management will be given are Enoxaparin 1x30 mg (0.3 cc) intravenous continue with 1x60 mg (0.6 cc) subcutaneous but because the Enoxaparin was out of stock, it changed by Fondaparinux 2,5 mg iv bolus followed by 2,5 mg subcutaneous, Ramipril 1X2.5 mg, Atorvastatin 1X40 mg, Alprazolam 1x5 mg, and Lactulax 1x15 cc. At the first, the patient was scheduled for Primary PCI but refused due to a health insurance problem. Then we performed fibrinolytic as alternative reperfusion therapy. Just about 15 minutes after fibrinolytic administrations, the patient became restless, shortness of breath, itchy, and rash all over his body. The blood pressure falls into 77/50 mmHg, respiration 32X/minute. The patient was then diagnosed with anaphylactic shock due to fibrinolytic drug. The patient was then managed by loading NaCl 0,9% 1000 cc, nebulization with combivent, and epinephrine 1mg subcutaneous and dexamethasone 8 mg intravenous. The patient's condition became stable again after 25 minutes of anaphylactic shock management was given. The patient was then moved to the cardiac catheterization lab for PCI intervention.
Discussion
Acute coronary syndrome
The acute coronary syndrome is an acute manifestation of coronary vascular atheroma plaque that is torn or ruptured due to changes in plaque composition and thinning of the fibrous layer covering the plaque. This event will be followed by platelet aggregation and activation of coagulation pathways so that platelet-rich thrombus is formed. This thrombus will fulfill the hole on coronary blood vessels, either completely or partially; or become a micro-embolism that fulfills distal coronary blood vessels. Reduced coronary blood flow causes myocardial ischemia. Inadequate either oxygen supply for approximately 20 minutes can cause an infarct on the myocardial [4].
STEMI diagnosis is established if there are acute angina pectoris complaints accompanied by persistent elevation ST-segment in 2-pairing lead ECG. The complaint of acute angina pectoris is a typical chest pain that includes a sense of oppressed/ heaviness on the retrosternal area, radiating to the www.jcimcr.org Page 3 left arm, neck, jaw, interscapular area, shoulder, or epigastric area. These complaints can last about intermittent (several minutes) or persistent (> 20 minutes). Typical angina complaints are often followed by other complaints such as sweats cold, nausea/vomiting, abdominal pain, shortness of breath, and fainting [4]. In our patient, persistent ST elevation segment on ECG is present [4].
Epidemiology
Although a rare occurrence, allergic reactions to the fibrinolytic agents have been described in the literature. Reactions more commonly occur following streptokinase administration but have been described with tissue-type Plasminogen Activator (tPA). Anaphylactoid reactions occur in up to 0.02% of patients treated for acute myocardial infarction and from 1.5% to 1.9% of those being treated for acute ischemic stroke [5].
Type 1 hypersensitivity Pathophysiology
Allergens (or antigens) are presented to T-cells by Antigen-Presenting Cells (APCs) during the sensitization phase of Type I hypersensitivity. T-cells then signal for stimulation of B-cells to produce IgE antibodies, which bind to the Fc receptors on mast cells and basophils. Subsequently, the free antigen induces the crosslinking of these mast cell and basophil bound IgE antibodies. This results in the degranulation of the cells and the release of histamine, proteolytic enzymes, and other mediators (i.e., prostaglandin, cytokines, leukotrienes, platelet-activating factors, macrophage inflammatory proteins, tryptase, etc.) [6].
As a result, there is increased vascular permeability, peripheral vasodilation, and smooth muscle contraction, which can manifest to increased mucous secretions, bronchospasm, abdominal cramping, rhinitis, and potentially hypovolemia or hypoxia. Pulmonary edema or general edema can also occur due to fluid shifting into interstitial space. Individuals can experience pruritis and local response of asthma or a systemic response of anaphylaxis [6].
Evidence for and against corticosteroid prophylaxis
Corticosteroid prophylaxis continues to be commonly used in the United States for the prevention of allergic reactions.
However, it has only a weak mitigating effect on allergic-like reactions, is unlikely to affect the severity of subsequent reactions, and does not prevent all reactions. Breakthrough reactions occur, can be life-threatening, and are usually the same severity as the index reaction. There is no evidence base to support the use of rapid prophylaxis regimens [7].
Preference consideration of reperfusion therapy
Immediate reperfusion therapy, both with PCI and pharmacologically, is indicated for all patients with onset symptoms within 12 hours with persistent ST segments elevation. Reperfusion therapy is also indicated if there is clinical or ECG evidence of ongoing ischemia even if symptoms have been present more than 12 hours from onset. In determining reperfusion therapy, the first step is determining the surrounding hospital has PCI facilities or not. When there are no PCI facilities, fibrinolytic therapy will immediately choose. If the PCI facilities are present, make sure the travel time from the site (hospital or clinic) to the hospital is less than 2 hours. If it takes more than 2 hours, then the reperfusion preference is fibrinolytic. Once fibrinolytic is completed, if possible the patient should be sent to the hospital with a PCI facility [4].
Fibrinolytic is an important reperfusion strategy, especially in medical services that cannot perform a primary PCI on STEMI patients on the recommended onset of time. Fibrinolytic therapy is recommended within 12 hours after onset manifestation without contraindication and primary PCI cannot be performed within 120 minutes onset of first medical contact. Fibrinolytic must be started in the emergency room [4].
Fibrin-specific agents (Tenecteplase, Alteplase, Reteplase) are more recommended than agents that are not specific to fibrin (Streptokinase). Oral aspirin should be administrated. Clopidogrel is indicated to be administered as an additional with aspirin. Anticoagulants are recommended in STEMI patients treated with fibrinolytic until revascularization (if performed) or during hospitalization for up to 5 days. Anticoagulants used can be Enoxaparin, UFH, or Fondaparinux. If a fibrinolytic failure (ST-segment resolution <50% within 60-90 minutes after fibrinolytic administration), or hemodynamic or electrolyte instability, worsening of ischemia, or persistent chest pain, is a condition with indications for PCI Rescue. If fibrinolytic success, routine coronary angiography is recommended [4].
The patient in this case is coming within 8 hours onset of manifestation and scheduled primary PCI. However, due to health insurance policies, the action was postponed while waiting for administrative issues to be resolved. While waiting, the patient performed fibrinolytic with Streptokinase 1.5 million units in 100 milliliter D5% or NaCl 0,9% drip intravenous within 30 – 60 minutes. After 15 minutes of fibrinolytic administration the patient looks restless, shortness of breath, itchy, and rash all over the body. The patient blood pressure decrease at 77/50mmHg, respiration 32x/minute. The patient was then diagnosed as in anaphylactic shock because of the fibrinolytic drug.
Management of anaphylactic shock
Anaphylactic patient with or without hypotension or shock, it is important to do a resuscitation with the normal saline maximum at 20 millimeters/kg BW within the first 30 minutes. Adrenaline is given as the first-line therapy in anaphylactic conditions and acts for reducing edema on respiratory mucosa, induce bronchodilation, induce vasoconstriction, and increases the strength of cardiac contraction. The adrenaline is given (Epinephrine) 1:1000 with 0,01 mg/kg BW until 0,5 mg/kg BW each dose, 5 minute interval every administration intramuscular. If after 2-3 administration the anaphylactic condition remains or getting worse, give adrenaline intravenous on 100millimeter of normal saline at a speed of 0,5 milimeter/KgBW/h using an infusion pump. In patients with shortness of breath condition accompanied by wheezing, nebulization is given with bronchodilator (Salbutamol 5mg nebulizer) and corticosteroid (oral prednisone 1 mg/kg BW maximum 50mg or Hydrocortisone 5 mg/kg BW intravenous maximum 200 mg) [8].
The patient in this case got loading NaCl 0,9% 1000 milliliter within the first 30 minutes, get 2-time epinephrine 0,5 mg intramuscular administration, nebulization with combivent, and Dexamethasone 8 mg intravenous (conversion from 200 mg hydrocortisone). The patient’s condition becomes stable after 25 minutes of anaphylactic shock management was given. The patient was then treated in intensive care for PCI.
Conclusion
STEMI is the most emergency condition that causes death. Reperfusion therapy needs to be done immediately to shorten the ischemic duration. Percutaneous Coronary Intervention is the gold standard of treatment in STEMI patients. However, we can not control other factors that might delay or it could not be done so we have to perform fibrinolytic therapy. Aside from common complications of fibrinolytic, this case-report aware us of an uncommon complication, anaphylactic shock.
References
- ESC. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. European Heart Journal. 2018; 39: 119-77.
- Bendary A, Tawfik W, Mahros M, Salem M. Fibrinolytic therapy in patients with ST-segment elevation myocardial infarction: Accelerated versus standard Streptokinase infusion regimen. J Cardiovasc Thorac Res. 2017; 9: 209-214.
- Duangmee K, Boonmuang P, Santimaleeworagun W, Prasitdumrong H. Urticaria, angioedema, and type I hyper sensitivity reactions associated with fibrinolytic agents. Asian Pac J Allergy Immunol. 2019.
- PERKI. Pedoman Tatalaksana Sindrom Koroner Akut. 2018.
- Mills GC, Arntfield RT, Sedran RJ. Acute allergic reaction due to the administration of fibrinolytic therapy for ST-segment elevation myocardial infarction: Case report and discussion. Can J Emerg Med. 2003; 5: 421-423.
- Abbas M, Moussa M, Akel H. Type I Hypersensitivity Reaction Treasure Island (FL): StatPearls Publishing: StatPearls. 2020.
- Davenport MS, Cohan RH. The Evidence for and Against Corticosteroid Prophylaxis in At-Risk Patients. Radiol Clin N Am. 2017; 55: 413-421.
- ASCIA. Guidelines Acute Management of Anaphylaxis. 2020.