Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Intra-cardiac cement embolism during hip arthroplasty
Alexander Amir1*; David Bracco2; Gabriele Baldini2; André Denault3
1Assistant Professor, Anesthesiology, McGill University Health Center, Canada.
2 Associate Professor, Anesthesiology, McGill University Health Center, Canada.
3 Professor Anesthesiology, Montreal Heart Institute, Université de Montréal, Montreal, Quebec, Canada.
*Corresponding Author : Alexander Amir
Assistant Professor, Anesthesiology, McGill University Health Center, Canada.
Email: Email: alexanderamir@gmail.com
Received : Apr 09, 2021
Accepted : May 05, 2021
Published : May 10, 2021
Archived : www.jcimcr.org
Copyright : © Amir A (2021).
Citation:Amir A, Bracco D, Baldini G, Denault A. Intra-cardiac cement embolism during hip arthroplasty. J Clin Images Med Case Rep. 2021; 2(3): 1128.
Clinical image description
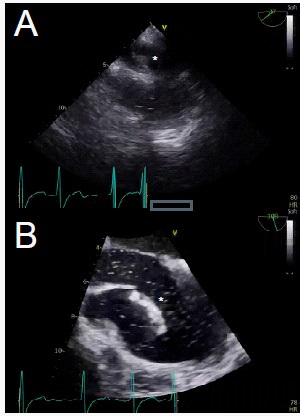
A 92-year-old woman presented to the operating room with a right femoral neck fracture. She had a past medical history significant for atrial fibrillation, coronary artery disease with a history of coronary bypass, severely stenotic aortic valve (area 0.9 cm2), diabetes, dyslipidemia, hypertension and dementia. She underwent general anesthesia with continuous Transesophageal Echocardiographic (TEE) monitoring for a right hemi-arthroplasty. While cementing the prosthesis, small cement emboli were initially seen (ME ascending aorta SAX view) migrating in the pulmonary artery (Figure A*). Subsequently, a large (4 cm) cement embolus was visualized in the right atrium, adhered to the Eustachian valve, an embryonic remnant (Figure B*, supplementary video A). The patient experienced no significant hemodynamic compromise or issue with gas exchange. Given embolization risk and severe potential for harm, intervention may be indicated. Treatment options were discussed but given hemodynamic stability, patient age and comorbidities, the patient was monitored without further intervention.