
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Hepatoportal Sclerosis in patient with Systemic Sclerosis and Sjögren’s Syndrome: a rare association
Giorgio Soardo1,2*; Maria Orsaria3; Laura Scatà11; Debora Donnini1; Leonardo A Sechi1
1Liver Unit, Internal Medicine, Department of Medicine (DAME), University School of Medicine of Udine, Udine, Italy.
2 Italian Liver Foundation, Basovizza (Trieste), Italy.
3 Institute of Pathological Anatomy, Department of Laboratory Medicine, University School of Medicine of Udine, Udine, Italy.
*Corresponding Author : Giorgio Soardo
Liver Unit, Internal Medicine, Department of Medicine (DAME), University School of Medicine of Udine, Piazzale Santa Maria della Misericordia 1, 33100 Udine-Italy.
Email: giorgio.soardo@uniud.it
Received : Apr 10, 2021
Accepted : May 06, 2021
Published : May 11, 2021
Archived : www.jcimcr.org
Copyright : © Soardo G (2021).
Abstract
We present the case of a 51 years-old woman who was referred to our Liver Unit for suspected dysmetabolic liver disease. She had a previous diagnosis of Systemic Sclerosis and Sjögren’s Syndrome and had altered hepatic enzymes with a positive anti-Nuclear Antibodies centromeric pattern, anti-Cardiolipin Antibodies and anti b2 Glycoprotein I Antibodies. Despite complete liver assessment and disease staging was negative, the clinical course was complicated by the development of anemia, due to esophageal varices bleeding associated with worsening splenomegaly. Liver biopsy was key for reaching the diagnosis as it showed portal tracts with fibrous expansion, ductular proliferation and focal lympho-granulocytic infiltrate, reduced caliber of portal vessels, hypoplastic portal tracts, focal herniation, aberrant microvasculature and positive endothelial CD34 staining. Having ruled out any other cause of portal hypertension such as cirrhosis, blood diseases, occlusion of the hepatic and portal veins, etc., we finally concluded that the portal hypertension was due to hepatoportal sclerosis associated with Systemic Sclerosis and Sjögren’s Syndrome.
Keywords: Idiopathic Non-Cirrhotic Portal Hypertension (INCPH; Hepatoportal Sclerosis (HPS); Systemic sclerosis (SSc); Sjögren’s Syndrome (SS).
Citation: Soardo G, Orsaria M, Scatà L, Donnini D, Sechi LA. Hepatoportal Sclerosis in patient with Systemic Sclerosis and Sjögren’s Syndrome: a rare association. J Clin Images Med Case Rep. 2021; 2(3): 1130.
Introduction
Hepatoportal Sclerosis (HPS) is a rare disease and a known cause of Idiopathic Non-Cirrhotic Portal Hypertension (INCPH). The clinical presentation is unspecific and is characterized by signs and symptoms of portal hypertension including splenomegaly and esophageal variceal bleeding, hematemesis, melena, anemia due to ruptured varices with normal liver function and a mild increase in liver enzyme concentration [1]. The diagnosis requires to rule out liver cirrhosis or preexisting portal vein thrombosis [2], but to show portal tracts enlarged by fibrosis, mega sinusoids and phlebosclerosis (portal vein wall thickening with a consequent luminal reduction) [3]. The characteristic histopathological lesions are often very mild and subtle, varying greatly in their severity, and not all are present in every case [4]. HPS is mainly reported in the Indian subcontinent [5] in males in their thirties or forties, and in Japan [6] and the West [7] in females in their fifties. In some patients we can find HPS in association with immunological disorders such as immunodeficiency [8], rheumatoid arthritis, systemic lupus erythematosus, scleroderma, celiac disease, Sjögren’s Syndrome (SS) [9]. Very few examples of association between HPS and Systemic Sclerosis (SSc) are described in the literature: In 2005 Kogawa et al. 10] presented a rare case of a 72 years-old Japanese woman with HPS associated with SSc and SS; and in 2006 Takagi et al. report a similar case with portal hypertension and SSc [11]. In 2014 the case of a female patient with atypical hepatic changes due to HPS with limited systemic sclerosis was referred in Brazil [12].
Case description
We present the case of a 51 years-old woman admitted to our Liver Unit in February 2019 for suspected dysmetabolic hepatic disease. At physical examination, vital parameters were in the normal range and the Body Mass Index (BMI) was 28 (kg/m2). Minimal facial telangiectasias and Raynaud’s phenomenon were present with no cutaneous signs of liver disease. The clinical history was notable for a diagnosis of Raynaud’s phenomenon in 1996, a long history of minimal alteration of necrosis and cholestatic hepatic enzymes associated with a positivity to Anti-Nuclear Antibodies (ANA) with a centromeric pattern, anti-Cardiolipin Antibodies (ACLA-IgM) and anti b2 Glycoprotein I Antibodies (b2GPI -IgM) (Table 1). A hepatic biopsy, performed in 2016, evidenced widespread, small and medium droplet steatosis, associated with mild chronic periportal inflammation with incomplete thin fibrotic periportal bridging. In 2017, a spirometry revealed a non-maximal PEF (Peak Expiratory Flow) due to a mild obstructive deficit, FVC (Forced Vital Capacity) =86%, FEV1 (Forced Expiratory Volume/1s) =74%, TLC (Total Lung Capacity) =96% and a medium degree deficit of the alveolus – capillary CO diffusion (DLCO=51%). In the same year a capillaroscopy showed findings consistent with an early scleroderma pattern, leading to a rheumatological diagnosis of Systemic Connective Tissue Disease due to the overlap of progressive Systemic Sclerosis (SSc) and Sjögren’s Syndrome (SS). In 2018 an abdominal ultrasound revealed a liver with normal echotexture, size and surface, without portal vein thrombosis or collateral vessels, and mild splenomegaly (DL=14 cm). In 2019 she was referred to our outpatient service for persistent alterations of cholestatic and hepatic necrosis enyzmes due to a suspected dysmetabolic disease and she underwent a complete diagnostic work up. HAV, HBV, HCV and HEV-RNA tests were negative, as well as serological markers of Autoimmune Hepatitis type I and type II and Autoimmune Biliary Disease. Wilson’s disease, genetic Haemochromatosis, Alfa-1 Antitrypsin deficiency, Porphyria, and Celiac disease were also rule out. Homeostatic Model Assessment for Insulin Resistance (HOMA) was in the normal range. A screening for the main risk factors for thrombophilia , including assessment of Antithrombin III, Factor V Leiden, activated C protein resistance, S protein, Prothrombin G20210A (Factor II Mutation), and Homocysteine was negative. The Erythrocyte Sedimentation Rate (ESR) was slightly increased (39 mm/h; NR=2-15 mm/h) whereas C Reactive Protein (CRP) and Complement (C3-C4) were in the normal range. Rheumatoid Factor (RF), the Extractable Nuclear Antigens (ENA) antibodies, anti-double-stranded DNA (anti ds-DNA) antibodies, Antineutrophil Cytoplasmic (ANCA) antibodies, Lupus Anticoagulant (LA) and Angiotensin Converting Enzyme (ACE) resulted negative. An Esophagogastroduodenoscopy (EGD) revealed no signs of esophageal varices; a Magnetic Resonance Cholangiography (MRC) evidenced signs of steatosis without any enlargement of the portal-splenic-mesenteric axes, no alterations in the biliary tree and an increase in splenomegaly (DL =15 cm). On December 2019 she came to the First Aid department of our hospital for hematemesis and melena with severe anemia (Hb= 4.9 g/dl; HCT=14%), and she underwent emergency sclerotherapy for rupture of a single esophageal varix. From February 2020 to November 2020 she was again in Day Hospital regimen at our department to study the variceal upper gastrointestinal bleeding, anemia and splenomegaly that, in association with Systemic Sclerosis, raised the suspicion of Idiopathic Non-Cirrhotic Portal Hypertension (INCPH). The EGD showed only scarring from the previous sclerotherapy. In June 2020, an abdominal ultrasound revealed normal hepatic size and structure with no portal occlusions, and increasing splenomegaly (DL=17,5cm); an MRC evidenced a mild increase in the hyperintense signal in the IV segment of the liver, possibly due to cholestasis or early fibrotic phenomena. At the same time Hepatic Venous Pressure Gradient (HVPG) measured by catheterization, the gold standard for measurement of portal pressure, revealed a mild abnormal HPVG of 7 mmHg (free hepatic venous pressure: 11 mmHg and wedged hepatic venous pressure: 18 mmHg). In September 2020 a new percutaneous liver biopsy was performed, which showed some portal tracts with fibrous expansion, ductular proliferation and focal lympho-granulocytic infiltrate. (Figure 1). Some portal vessels resulted reduced in caliber, portal traits appeared hypoplastic, with defined vascular structures, focal herniation (Figure 2 a,b) and aberrant microvasculature. We noticed the presence of dilated, irregular vessels at the periphery of the portal tracts. (Figure 3). The hepatocytes showed macro-vesicular steatosis in about 20% of the cells. There was no evidence of iron deposition. Sinusoidal dilation was a frequent pattern, sometimes with perisinusoidal fibrosis and sinusoidal capillarization with aberrant expression of CD34 (Figure 4 a,b,c). Having reexamined the specimen of 2016 liver biopsy available, we performed a retrospective histopathologic examination searching for early signs of hepatoportal fibrosis. As showed in Figure 5, in 2016 there were no significant signs of altered portal spaces, except for minimal vascular dilatation. However, CD34 immunostaining highlighted initial signs of sinusoidal capillarization (Figure 6).
Considering the clinical history, the HVPG measurement, the absence of other causes of liver cirrhosis and portal vein thrombosis, and most importantly the histological findings, we concluded that the patient had portal hypertension caused by HPS due to the overlap of systemic sclerosis and Sjögren’s syndrome.
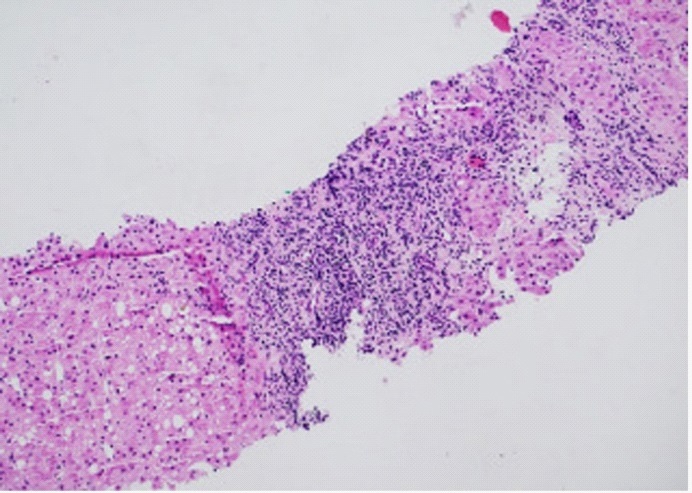
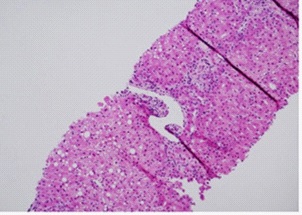
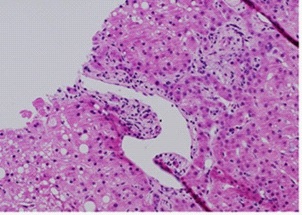
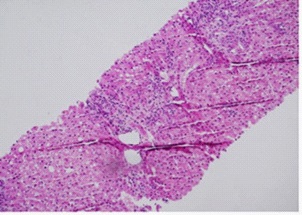
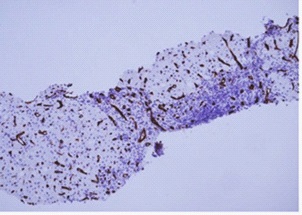
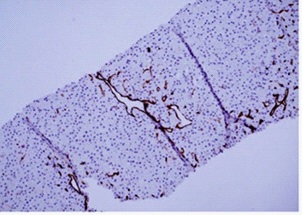
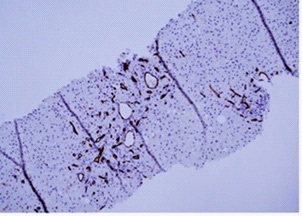
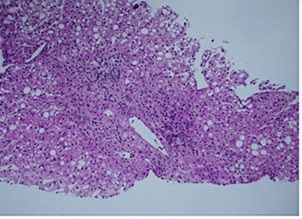
Table 1: Significant test results of the patient over the years.
Laboratory tests |
Normal Range |
Year 2011 |
Year 2016 |
Year 2019 |
Year 2020 |
AST |
(5-40) U/L |
55 |
53 |
46 |
57 |
ALT |
(5-40) U/L |
79 |
73 |
47 |
82 |
GGT |
(6-39) U/L |
103 |
115 |
148 |
195 |
LAP |
(35-104) U/L |
92 |
136 |
224 |
248 |
Total Bilirubin |
(0.20-1.00) mg/dL |
1.19 |
1.12 |
0.87 |
1.13 |
PT/INR |
(0.8-1.20) |
1.02 |
1.02 |
1.05 |
1.03 |
Platelet count |
(150-400) 103/µL |
219 |
141 |
110 |
81 |
Hb |
(12.0-16.0) g/dL |
13.5 |
12.0 |
11.9 |
12.5 |
Albumin |
(35-50) g/L |
44.6 |
44.0 |
44 |
42.6 |
ANA (centromeric pattern) |
negative |
1:1280 |
1:2560 |
1:5120 |
1:2560 |
ACLA-IgM |
(0 – 7) UI/ml |
13 |
28 |
45 |
57 |
b2GPI -IgM |
(0 – 8) UI/ml |
11 |
29 |
42 |
59 |
ANA: Anti - Nuclear Antibodies; ACLA: Anti-Cardiolipin Antibodies; b2GP-I: Anti b2 Glycoprotein I Antibodies.
Discussion
Obliterative portal venopathy, non-cirrhotic portal fibrosis and nodular regenerative hyperplasia define a disease entity with heterogeneous morphological features, now grouped under the term of Idiopathic Non-Cirrhotic Portal Hypertension (INCPH) [13], a vascular liver disease characterized by unknown etiology and a diagnosis obtained after exclusion of all known causes of chronic liver disease. In particular it requires the following criteria: 1) presence of clinical signs of portal hypertension such as splenomegaly and/or hypersplenism, esophageal and/or gastric varices, ascites (nonmalignant), portal venous collaterals; 2) exclusion of liver cirrhosis at biopsy; 3) exclusion of chronic liver disease that may cause non-cirrhotic portal hypertension, such as chronic hepatitis B or C virus infection, Wilson disease, primary biliary cholangitis, non-alcoholic steatohepatitis, autoimmune hepatitis, congenital liver fibrosis, sarcoidosis, myeloproliferative disease, hepatic arterioportal shunts etc.; 4) presence of liver imaging showing patent portal and hepatic veins [14]. HPS is one of the known causes of INCPH and it is characterized by presinusoidal intrahepatic portal hypertension associated with splenomegaly and anemia in patients with a non-cirrhotic liver. The histological features are obliterative portal venophaty of the small portal veins, periportal /perisinusoidal fibrosis, dilated portal vascular spaces and thickened or sclerotic portal veins with herniation in the surrounding parenchyma, in the absence of cirrhosis [15,16]. Some studies suggest an autoimmune etiology in a fraction of cases, since a higher incidence has been noticed in patients with connective tissue diseases as in our patient [10,11,17]. In patients with SSc, enhanced fibrogenesis seems to have a major pathogenic role [18]. Fibrogenesis is a multistage process, caused by deregulated tissue repair responses whereby aberrantly sustained production of cytokines, growth factors, and angiogenic factors tilt tissue homeostasis towards interstitial hyperplasia and excessive accumulation of extracellular matrix [19]. Injury to vascular endothelial cells followed by disrupted or inappropriate repair processes could lead to sclerosis of the intrahepatic vessels [20]. In our patient the admission to our Liver Unit was related to a suspect of a dysmetabolic liver disease. However, as shown in Table I, the main liver markers were slightly altered and did not increase over the years. On the other side, the positivity to ANA, ACLA-IgM and b2GPI -IgM were increasing and all the other findings lead to a diagnosis of a systemic sclerosis overlapped to a Sjögren’s syndrome. One study [21] reported a positive correlation between portal inflammation and ANA and between sinusoidal fibrosis and transaminases, while platelets were inversely correlated with sinusoidal dilatation, increased central veins and diffuse sinusoidal capillarization. These findings were present in our patient at admission (Table 1) and they could have led us to a suspicious of HPV. However, only one year later, did we have clear signs of portal hypertension: anemia, bleeding esophageal varices and an increase in splenomegaly. The study of the liver with abdominal ultrasounds, abdominal MRI and MRC excluded all known causes of portal hypertensions. Thus, the histological examination of the liver tissue samples became crucial to achieve a definite diagnosis of HPS. The characteristic lesions include inconspicuous portal tracts, incomplete or complete obliteration of portal vein branches and/or thickening of the wall, or fibrous expansion of portal tracts [22]. Alternately we can find dilation of vessels in/or near portal tracts with an increased number of thin-walled vascular spaces, often without an effective portal vein. Portal vascular spaces directly abutting upon the hepatic parenchyma at the limiting plate are a frequent finding (herniated portal vein). Sinusoidal dilation is often present, sometimes with perisinusoidal fibrosis and sinusoidal capillarization [22]. The structural characteristics of hepatic sinusoids are gradually lost during the process of so-called “Capillarization” that accompanies the evolution of chronic liver diseases such as hepatoportal fibrosis. Intrahepatic angiogenesis and sinusoidal remodeling often occur and are characterized by the deposition of a basement membrane, the loss of sinusoidal endothelial fenestrae, and by the expression of CD34 (commonly referred to as the capillarization of sinusoids) [23]. But even if liver biopsy is essential for a diagnosis, especially at early stages, the histological findings can be heterogeneous and difficult to interpret. In fact, in our patient, the histological examination of the liver at the early stage of the disease (2016) was not conclusive and the presence of a mild chronic periportal inflammation with incomplete thin fibrotic periportal bridging was underestimated. Only when we had clear signs of portal hypertension (anemia, bleeding esophageal varices), did the liver biopsy show different degrees of fibrosis, portal or peri-portal thickening, with intimal sclerosis and thrombosis of small intrahepatic portal branches. These histological finding, the HVPG measurement [24] together with the absence of other causes of cirrhosis, portal vein thrombosis, necrosis or inflammatory phenomena in the liver finally led to the final diagnosis: HPS associated with systemic sclerosis and Sjögren’s syndrome. The diagnosis was long and difficult because hepatoportal sclerosis is rare, but this did not change the prognosis and survival of our patient since HPS evolves very slowly. Furthermore, there are no specific therapies for HPS, except the prophylaxis and treatment of esophageal varices which are the main cause of morbidity and mortality in these patients. Further studies are necessary to establish the correlation between HPS, SSc and SS since Salliot et al. [25] failed to demonstrate that SS is secondary to SSc and in literature we found cases of association of HPS with SSc [11,12,26-28] or with SS [29,30]; but we found only one case of HPS associated with both SSc and SS in a Japanese female patient [10].
Conclusions
In this case report we want to underline the difficulties encountered in diagnosing HPS in a patient with a preexisting diagnosis of SSc and SS. She was admitted to our Liver Unit to complete a diagnostic work up for a persistent and variable alteration of cholestatic and hepatic necrosis attributed to a possible dysmetabolic disease. We performed all the diagnostic procedures recommended by the protocol for the study of the liver, but we had no reason to suspect portal hypertension until the patient manifested anemia, bleeding esophageal varices and an increase in splenomegaly. The histological examination of the liver showed all the signs of HPS and we finally arrived at the diagnosis of “portal hypertension caused by HPS associated with Systemic Sclerosis and Sjögren’s Syndrome”. Clinicians should be aware of this very rare association of SSc and SS with idiopathic non-cirrhotic portal hypertension to avoid misdiagnosis.
References
- Bioulac-Sage P, Le Bail B, Bernard PH, Balabaud C. Hepatoportal sclerosis. Semin Liver Dis. 1995; 15:329-339.
- De Gottardi A, Rauton PE, Schouten JN, Rubbia-Brandt L, Leebeek F, et al. Porto-sinusoidal vascular disease: Proposal and description of a novel entity. Lancet Gastroenterol Hepatol. 2019; 4: 339-411.
- Mikkelsen WP, Edmonson HA, Peters RL, Redeker AG, Reynolds TB. Extra-and intrahepatic portal hypertension without cirrhosis (hepatoportal sclerosis). Ann Surg. 1965; 162: 602-620.
- Nayak NC, Jain D, Saigal S, Soin AS. Non-cirrhotic portal fibrosis: One disease with many names? An analysis from morphological study of native explant livers with end stage chronic liver disease. J Clin Pathol. 2011; 64: 592–8.
- Madhu K, Avinash B, Ramakrishna B, Eapen CE, Shyamkumar NK, et al. Idiopathic non-cirrhotic intrahepatic portal hypertension: common cause of cryptogenic intrahepatic portal hypertension in a Southern Indian tertiary hospital. Indian J Gastroenterol. 2009; 28: 83-87.
- Aoki H, Hasumi A, Joshida K. A questionnaire study on treatment of idiopathic portal hypertension and extrahepatic portal obstruction. Kameda H editor. Annual report on portal hemodynamics abnormalities. Tokyo: Japan Ministry of Health and Welfare. 1988; 179-189.
- Hillaire S, Bonte E, Denninger MH, Casadevall N, Cadranel JF, et al. Idiopathic non-cirrhotic intrahepatic portal hypertension in the West: A re-evaluation in 28 patients. Gut 2002; 51: 275-280.
- Song J, Lleo A, Yang GX, Zhang W, Bowlus CL, et al. Common variable immunodeficiency and liver involvement. Clin Rev Allergy Immunol. 2018; 55: 340-351.
- Fiel IM, Thung SN, Hytiroglou P, Emre S, Schiano TD. Liver failure and need for liver transplantation in patients with advanced hepatoportal sclerosis. Am J Surg Pathol. 2007; 31: 607–614.
- Kogawa H, Migita S, Ito M, Takii Y, Daikoku M, et al. Idiopathic portal hypertension associated with systemic sclerosis and Sjögren’s Syndrome. Clin Reumatol. 2005; 24: 544-547.
- Takagi K, Nishio S, Akimoto K, Yoshino T, Kawai S. A case of systemic sclerosis complicated by idiopathic porta hypertension: Case report and literature review. Mod Reumatol. 2006; 16:183-187.
- Ortega Espinosa CR, Saldarriaga Rivera LM. Presentation of Idiopathic Portal Hypertension in a patient with Limited Systemic Sclerosis. Rev Col Gastroenterol. 2014; 29: 269-273.
- Schouten JN, Garcia-Pagan JC, Valla DC, Janssen HL. Idiopathic noncirrhotic portal hypertension. Hepatology. 2011; 54: 1071–1081.
- Schouten JN, Verheij J, Seijo S. Idiopathic non-cirrhotic portal hypertension: A review. Orphanet J Rare Dis. 2015; 10: 67.
- Nakanuma Y, Hoso M, Sasaki M, Terada T, Katayanagi K, et al. Histopathology of the liver in non-cirrhotic portal hypertension of unknown aetiology. Histopathology. 1996; 28: 195-204.
- Khanna R, Sarin SK. Non-Cirrhotic Portal Hypertension: current and emerging perspectives Clin Liver Dis. 2019; 23: 781-807.
- Horai Y, Miyamura T, Hirata A, Nakamura M, Takahama S, et al. Idiopathic Portal Hypertension in a patient with Mixed Connective Tissue Disease and Protein C deficiency. Inter Med. 2010; 49: 2013-2016.
- Moschos J, Leontiadis GI, Kelly C, Henry J, Kadis S. Idiopathic portal hypertension complicating systemic sclerosis: A case report BMC Gastroenterol. 2005; 5: 16.
- Ho YY, Lagares D, Tager AM, Kapoor M. Fibrosis - a lethal component of systemic sclerosis. Nat Rev Rheumatol. 2014; 10: 390–402.
- Sato Y, NakanumaY. Role of endothelial-mesenchymal transition in idiopathic portal hypertension. Histol Histophatol. 2013; 28: 145-154.
- Guido M, Sarcognato S, Sonzogni A, Lucà MG, Senzolo M, et al. Obliterative portal venopathy without portal hypertension: An underestimated condition. Liver Int. 2016; 36: 454–460.
- Guido M, Alvares VAF, Balabaud C, Bathal PS, Bioulac-Sage P, et al. Histology of portal vascular changes associated with idiopathic non-cirrhotic portal hypertension: Nomenclature and definition. Histopathology 2019; 74: 219-226.
- Poisson J, Lemoinne S, Boulanger C, Durand F, Moreau R, et al. Liver sinusoidal endothelial cells: Physiology and role in liver diseases. J Hepatol. 2017; 66: 212-227.
- Alonso S, Bañares R, Barrio J, Rincón D, Nuñez O, et al. Utilidad diagnóstica del estudio hemodinámico hepático en la esclerosis hepatoportal. Gastroenterol Hepatol. 2001; 24: 473-477.
- Salliot C, Mouthon L, Ardizzone M, Sibilia J, Guillevin L et al. Sjogren’s syndrome is associated with and not secondary to systemic sclerosis. Rheumatology (Oxford). 2007; 46: 321-326.
- Morris JS, Htut T, Read AE. Scleroderma and portal hypertension. Ann Rheum Dis. 1972; 31: 316-318.
- Umeyama K, Yui S, Fukamizu A, Yoshikawa K, Yamashita T. Idiopathic portal hypertension associated with progressive systemic sclerosis. Am J Gastroenterol. 1982; 77: 645-648.
- Tsuneyama K, Harada K, Katayanagi K, Watanabe K, Kurumaya H, et al. Overlap of idiopathic portal hypertension and scleroderma: Report of two cases and a review of literature. J Gastroenterol Hepatol. 2002; 17: 217-223.
- Kitamura Y, Tsukada N, Atsukawa K, Shinagawa J, Yonei Y, et al. A case of non-cirrhotic portal hypertension complicated with Sjogren’s syndrome and thrombocytosis. Nippon Shokakibyo Gakkai Zasshi. 1995; 92: 95-100.
- Cazals-Hatem D, Hillaire S, Rudler M, Plessier A, Paradis V, et al. Obliterative portal venopathy: Portal hypertension is not always present at diagnosis. Journal of Hepatology. 2011; 54: 455–461.