
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Sudden onset hearing and visual loss: An unusual presenting manifestation of chronic phase chronic myeloid leukaemia
Sneha Tandon1*; Sanjeev Yadav2; Ruchi Gupta2; Soniya Nityanand2
1Division of Paediatric Oncology, Department of Paediatrics, University Hospital Southampton, Southampton, United Kingdom.
2Department of Haematology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India.
*Corresponding Author : Sneha Tandon
Division of Paediatric Oncology, Department of Paediatrics, University Hospital Southampton, Southampton, United Kingdom.
Email: sneha.tandon@uhs.nhs.uk
Received : Apr 12, 2021
Accepted : May 06, 2021
Published : May 11, 2021
Archived : www.jcimcr.org
Copyright : © Tandon S (2021).
Citation: Tandon S, Yadav S, Gupta R, Nityanand S. Sudden onset hearing and visual loss: An unusual presenting manifestation of chronic phase chronic myeloid leukaemia. J Clin Images Med Case Rep. 2021; 2(3): 1133.
Introduction
Chronic Myeloid Leukaemia (CML) commonly presents with generalized weakness, splenomegaly, leucocytosis with basophilia, while neurological manifestations like convulsions, hearing loss, papilledema are rare. Moreover, hearing and or vision loss is seldom encountered as a primary manifestation [1-6], with various mechanisms implicated for vascular obstruction and end organ dysfunction [4]. We hereby, report a retrospective series of six patients with CML in Chronic Phase (CP) who presented with visual loss and/or Sensorineural Hearing Loss (SNHL). Due to the rarity of this presentation we feel our case series could contribute to the existing scarce literature.
A detailed history and clinical examination including auditory and ophthalmological evaluation were performed in each patient. Related radiological evaluation was done as needed. Data was recorded by reviewing the electronic medical records and patient charts. All patients were given imatinib as first line Tyrosine Kinase Inhibitor (TKI). Pure Tone Audiometry (PTA) and fundoscopy were performed at diagnosis and repeated post one month of treatment with imatinib. Patients were followed-up as per standard international guidelines.
Clinical features and treatment (Table 1)
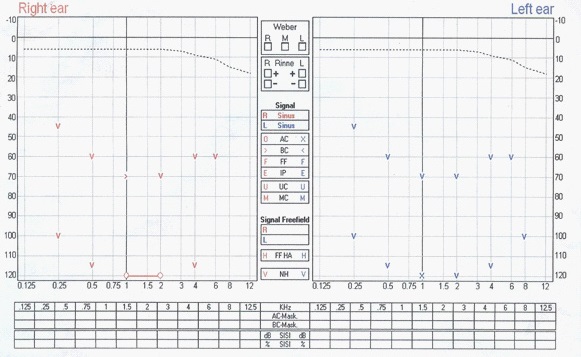
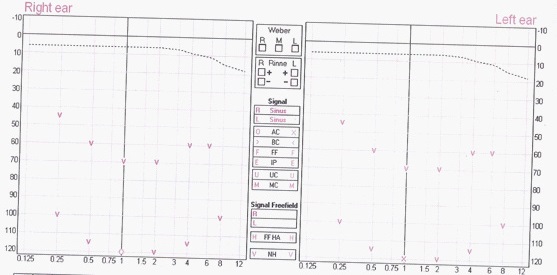
All six patients presented with acute onset visual and or hearing loss. Hearing loss was present at diagnosis in all patients at diagnosis, except patient 4 who was previously diagnosed with CML-CP and was on treatment with imatinib, however, had poor compliance to therapy. Splenomegaly and/or hepatomegaly and hyperleukocytosis was noted in all six patients. In 3 patients (patient 1,2 & 3), the profound hearing loss was accompanied by visual loss also. All six patients had bilateral moderate to profound SNHL (Figure 1a), which persisted despite therapy (Figure 1b), except in patient 3 wherein repeat testing was unavailable as patient was lost to follow-up. Retinal haemorrhages were noted in all patients with visual loss which reversed during follow-up. All patients received hydroxycarbamide for initial cytoreduction, except patient 4 and were subsequently commenced on imatinib (Table 1). After a follow-up of eight years, all patients (except patient 3) are doing well on treatment with imatinib for CML-CP, however, have persistent hearing loss.
Laboratory findings at diagnosis
The mean White Cell Count (WBC) at diagnosis was 611.5 x 109/L (range,264-850). Bone marrow morphology confirmed a diagnosis of chronic myeloid leukaemia in chronic phase in all patients. PTA revealed severe SNHL in all patients. MRI head was done in 4/6 patients and was normal except in patient 1 where it showed multiple cerebral haemorrhages with normal cochlea, VII and VIII cranial nerve complex (Table 1).
Table 1: Patient characteristics.
Patient |
Age |
Sex |
Presenting manifestations |
Highest White Cell Count(WBC) count (109/L) |
Pathological diagnosis/stage |
Salient Investigations |
Management and Outcome |
1 |
36 |
M |
Fever,generalized weakness,hepatomegaly, splenomegaly, bilateraldiminution of vision and hearing (<7d), Fundoscopy bilateral pre-retinalhaemorrhagesinvolving macula, Roth’s spots and exudative lesions, blockedretinal vessels |
700 |
CML-CP |
Pure tone audiometry: MRI brain |
Hydroxycarbamide (10days),single LPIT methotrexate, prednisolone (40mg/m2/d for 5 days), imatinib 400mg/d, switched to nilotinib due to failure to achieve CCyR, |
2 |
35 |
M |
Nausea, early satiety, Fundoscopy |
719 |
CML-CP |
Pure tone audiometry: MRI head |
Hydroxycarbamide, imatinib 400mg/d |
3 |
56 |
M |
Fever,decreased appetite Fundoscopy |
586 |
CML-CP |
Pure tone audiometry: Bilateralprofound SNHL |
Hydroxycarbamide, imatinib 400mg/d |
4 |
26 |
M |
Previously diagnosed with CML -CP, on treatment developed sudden, severe bilateral hearing loss, splenomegaly |
264 |
CML-CP |
Pure tone audiometry: bilateral SNHL |
Imatinib 400mg/d, increased to 800mg/d Bilateral persistent profound SNHL |
5 |
52 |
F |
Weakness, easy fatigue, abdominal discomfort for 2 months Splenomegaly (8 cm), hepatomegaly(3 cm) |
550 |
CML-CP |
Pure tone audiometry: bilateral SNHL MRI brain: Normal |
Hydroxycarbamide Bilateral persistent profound SNHL |
6. |
32 |
M |
Intermittent abdominal pain, early satiety, splenomegaly, bilateral hearing loss and vertigo(<7d). |
850 |
CML-CP |
Pure tone audiometry: bilateral profound SNHL MRI head: normal |
Hydroxycarbamide Bilateral persistent SNHL |
Discussion
Visual or hearing loss are rare clinical manifestations of CML with 29 cases reported [7,9-17]. Deafness as the presenting symptom is even rarer in CML-CP, with bilateral moderate-profound SNHL seen in all our patients. Various mechanisms have been implicated in the pathogenies of these symptoms, namely; leukemic infiltration of temporal bone or cochlea, hyperleukocytosis and hyperviscosity syndrome, inner ear haemorrhage and infection. Leukostasis and haemorrhage into the labyrinth and cochlea have been reported with bilateral hearing loss in CML [8,11,17-19]. Hyperleukocytosis, leucostasis and partial occlusion in the small calibre labyrinthine artery which supplies the cochlea and vestibular apparatus is the commonest incriminating factor in the pathogenesis [4]. Further, high oxygen consumption by leukemic cells competes for this precious resource in the microcirculation contributing to local tissue hypoxia and infarction. Even temporary stasis can cause irreversible damage to the delicate neuronal and vascular structures of the inner ear [20]. Moreover, the cochlea does not have its redundant blood supply and even brief periods of ischemia could lead to hearing loss [20]. Hyperleukocytosis as a cause for deafness is supported by cases showing recovery of hearing post leukapheresis [9,16].
It has been reported previously that the leukemic cells in CML may have a predilection for the labyrinth [21]. Myeloid lineage leukemic cells are larger and are unable to deform and pass through the microcirculation in the cochlea, thereby clogging the capillary microcirculation causing tissue hypoxia, infarction and permanent damage [19,20]. Leucostatsis and cerebral haemorrhage involving bilateral temporal and temporoparietal lobes can cause cortical deafness. Damage to the primary auditory complex leads to interruption of the projection fibres from the medial geniculate bodies to the auditory-related areas, culminating into severe, persistent hearing loss [18,22]. This can also be extrapolated to the visual loss associated with hyperleukocytosis and increased blood viscosity, which causes clogging of the end arterial supply of the retinal blood vessels and ischemic damage.
Hyperleukocytosis was seen in all patients and is likely to have contributed to the clinical manifestations. The MRI in 5/6 patients showed normal auditory nerve complex with no evidence of cochlear involvement or middle ear pathology. Patient 4 had a WBC of 264 x109/L despite being on imatinib irregularly for past five years without monitoring of transcript levels. Irreversible SNHL secondary to imatinib has been previously reported within three months of therapy initiation, with persistence despite cessation of imatinib [23], and thus it could be argued in him that there is a possibility of TKI induced hearing loss. However, contrary to this case-report, a single-centre cross-sectional study on 44 patients who had taken TKI for at least six months failed to depict an increased risk of audio-vestibular dysfunction at a median follow-up of 36 month [24]. Due to his unaffordability for second generation TKI, the dose of Imatinib was increased to 800 mg, on which he did well without worsening of his hearing loss, thus pointing towards Imatinib to be the unlikely cause of deafness.
In all our patients, we instituted prompt and aggressive cytoreductive treatment with hydroxycarbamide, however, only vision improved but SNHL persisted in all patients. Similar to our observation, previous case reports have also demonstrated that various interventions like hydroxycarbamide, low dose cytarabine, dexamethasone, intrathecal methotrexate, intra tympanic steroids have been unsuccessful in reversing the hearing loss [10,17]. Two reports have shown a beneficial role of leukapheresis [9,16], while others have not [17,25-27]. Thus, current literature shows irreversibility of SNHL in the majority of the cases [10,17], highlighting that an irreparable damage to the inner ear or auditory area in the brain occurs rapidly, and an early diagnosis and aggressive cytoreductive intervention is warranted.
Conclusion
In summary, this report highlights the unusual presentation with visual loss and SNHL in CML-CP. Our cases in corroboration with published literature show that the hearing loss associated with CML is irreversible in the majority of the cases. This has prognostic implications as well as highlights the irreparable rapid damage which occurs to the cochlea due to leucostasis. Thus, there should be a high index of suspicion of CML associated SNHL in any patient with sudden hearing loss and hyperleukocytosis that warrants aggressive cytoreductive therapy.
References
- Andres E, Kurtz JE, Maloisel F, Dufour P. Otological manifestations of acute leukaemia: Report of two cases and review of literature. Clin Lab Haematol. 2001; 23: 7–60.
- Rabinowitz I, Larson RS, Greer JP, Foerster J, Lukens JN, et al. Wintrobes clinical hematology. Lippincott Williams and Williams. 11th ed Lippincott. 2004; 2: 2235-2244.
- Pemmaraju N, Kantarjian H, Shan J, Jabbour E, Cardama AQ, VerstovsekS, et al. Analysis of outcomes in adolescents and young adults with chronic myelogenousleukaemia treated with upfront tyrosine kinase inhibitor therapy. Haematologica. 2012; 97: 1029-1035.
- Baer MR, Stein RS, Dessypris EN. Chronic lymphocyticleukemia with hyperleukocytosis. The hyperviscosity syndrome. Cancer. 1985; 15: 2865–2869.
- Chae SW, Cho JH, Lee JH, Kang HJ, Hwang SJ. Sudden hearing loss in chronic myelogenous leukaemia implicating thehyperviscosity syndrome. J LaryngolOtol. 2002; 116: 291–293.
- Chim CS, Woo JKS. Deafness in chronic myeloid leukaemia. Leuk Lymphoma. 1997; 26: 209–210.
- Genden EM, Bahadori RS. Bilateral sensorineural hearing loss as a first symptom of chronic myelogenous leukaemia. OtolaryngolHead Neck Surg. 1995; 113: 499–501.
- Gotay V. Unusual otologic manifestation of chronic lymphocyticleukemia. Laryngoscope. 1976; 86: 1856–1863.
- Resende LS, Coradazzi AL, Rocha-Junior C, Zanini JM, Niero-Melo L. Sudden bilateral deafness from hyperleukocytosis in chronic myeloid leukaemia. Acta Haematol. 2000; 104: 6–9.
- Naithani R, Chandra J, Mathur NN, Narayan S, Singh V. Hearing loss in chronic myeloid leukaemia. Pediatr Blood Cancer. 2005; 45: 54-56.
- Veling MC, Windmill I, Bumpous JM. Sudden hearing loss as a presenting manifestation of leukaemia. Otolaryngol Head NeckSurg. 1999; 120: 954–956.
- Rosa RH and Cunningham RD. Retinopathy of blood dyscrasias. Duane’s Clinical Ophthalmology. 2006; 2.
- Leonardy NJ, Rupani M, Dent G et al. Analyses of 135 autopsy eyes for ocular involvement in leukaemia. Am J Ophthalmol. 1990; 190: 436–444.
- Kanyike FB, Kigonya RM. Nerve deafness, dysarthria and ataxia in chronic granulocytic leukaemia - A case report. East Afr Med J. 1982; 596: 420–424.
- Huynh TH, Johnson MW, Hackel RE. Bilateral proliferative retinopathy in chronicmyelogenous leukemia. Retina. 2007; 27: 124-125.
- Gokce M, Unal S, Bayrakci B, Tuncer M. Chronic myeloid leukemia presenting with visual and auditory impairment in an adolescent: An insight to management strategies. Indian J Hematol Blood Transfus. 2010; 26: 96-98.
- Tsai CC, Huang CB, Sheen JM, Wei HH, et al. Sudden Hearing loss as the initial Manifestation of Chronic Myeloid Leukemia in a Child.Chang Gung Med J. 2004; 27: 629-633.
- Tanaka Y, Kamo T, Yoshida M, YamadoriA. So called cortical deafness: Clinical, neurophysiological and radiological observations. Brain. 1991; 114: 2385-2401.
- Genden EM, Bahadori RS. Bilateral sensorineural hearing loss as a first symptom of chronic myelogenous leukaemia. Otolaryngeal Head Neck Surg. 1995; 1134: 499-501.
- Mudry A, Tange R. The vascularization of the human cochlea: its historical background. Acta Otol. 209; 129: 3-16.
- Yamada K, Kaga K, Suzuki J. Temporal bone pathology in patients without caloric response. Acta Otolaryngol. 1994; 114: 586-594.
- Alimam SM, Mamat MK, Kulkarni S, Tim CP. Somervaille. British Journal of Hematology. 2012; 160: 3.
- Attili VSS, Bapsy PP, Anupama G, Lokanatha D. Irreversible sensorineural hearing loss due to imatinib. Leuk Res. 2008; 32: 991-992.
- Gupta R, Yanamandra U, Gupta B, Panda NK, Varma S, et al. Audio Vestibular Status in CML patients on Imatinib Mesylate with Review of Literature. Indian J Hematol Blood Transfus. 2017; 33: 175-180.
- Hsu YC, Su CY, Hsu RF. Unilateral sudden hearing loss as a presenting manifestation of chroniv myeloid leukemia: Case report. Otolaryngology-Head and Neck Surgery. 2004; 130: 271-273.
- Acar GO, Acioglu E, Enver O, Ar C, Sahin S. Unilateral sudden hearing loss as the first sign of chronic myeloid leukemia. European Archives of Oto-Rhino -Laryngology. 2007; 264: 1513-1516.
- Alimam SM, Mamat MK, Kulkarni S, Somervaille TCP. Sudden onset bilateral deafness as a presentation of chronic myeloid leukaemia. Br J Haematol. 2013; 160: 3.