
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Intraoperative trans-esophageal echographic evaluation of the celiac artery flow after arcuate ligament resection in a case of Dunbar Syndrome. A case report
Giacomo Coppalini1,2; Enrico Giustiniano2*; Fulvio Nisi2; Carlo Castoro1; Maurizio Cecconi1,2
1Humanitas University, Department of Biomedical Sciences, Via Rita Levi Montalcini 4, 20090 Pieve Emanuele, Milan, Italy.
2Humanitas Clinical and Research Hospital IRCCS, Department of Anesthesia and Intensive Care Units, Via Manzoni 56, 20089, Rozzano, Milan, Italy.
*Corresponding Author : Enrico Giustiniano
IRCCS-Humanitas Clinical and Research Hospital, Department of Anesthesia and Intensive Care Units, Via Manzoni 56, 20089, Rozzano, Milan, Italy.
Email: enrico.giustiniano@humanitas.it
Received : Apr 13, 2021
Accepted : May 10, 2021
Published : May 13, 2021
Archived : www.jcimcr.org
Copyright : © Giustiniano E (2021).
Keywords: Rare disease; Trans-esophageal echography; Celiac Trunk.
Citation: Coppalini G, Giustiniano E, Nisi F, Castoro C, Civilini E, et al. Intraoperative trans-esophageal echographic evaluation of the celiac artery flow after arcuate ligament resection in a case of Dunbar Syndrome. A case report. J Clin Images Med Case Rep. 2021; 2(3): 1137.
Introduction
Dunbar Syndrome (DS), also known as Median Arcuate Ligament (MAL) syndrome, is a rare disease in which the celiac trunk is compressed by a fibrous attachment at the diaphragmatic crura causing abdominal angina with a large spectrum of symptoms including nausea, vomiting, weight loss, and postprandial epigastric pain.
First anatomically described by Lipshutz in 1917 [1], this syndrome has a prevalence of 2/100,000 patients, women being more affected than men (3:1 ratio). DS usually involves young adults aged between 18 and 30 years. The traditional onset of the disease includes weight loss, nausea with vomiting, diarrhea and epigastric pain [2]. The MAL is a band of fibrous tissue that surrounds the aortic hiatus which can predispose to DS in case of higher origin or lower insertion on the diaphragm. This finding is significant in a small subset of patients, leading to compression of the celiac trunk during expiration, and relief during deep breath inspiration.
The pathophysiologic mechanism of this rare disease still remain unclear, but the most widely accepted theory suggests the post prandial increased demand for blood flow by the gut through a compressed celiac artery ultimately leads to transitory intestinal ischemia and epigastric pain. Possibly, chronic pressure on the celiac ganglion by the MAL can be associated with the development of neuropathic pain due to an overstimulation and irritation of sympathetic pain fibers triggering epigastric pain [2].
Color Doppler Ultrasounds (US) has shown a pivotal role for the diagnosis and follow-up of DS allowing the examiner to perform a dynamic study of the involved anatomical site. In previous case reports [3], echography has been used to confirm the return to normal flow on the celiac trunk after laparoscopic resection of the MAL, but never by means of trans-esophageal probe and intra-operatively.
With this case report we propose a novel application of the trans-esophageal echography not only as a diagnostic tool, but also as a functional guide during the surgical treatment of the DS and as a way to confirm the successful decompression of the celiac artery at the end of the operation.
Case report
An 18-year-old female patient was referred to the vascular surgery unit of our Hospital suffering from post-prandial abdominal angina and weight loss, suggestive of DS.
She had a 1-year history of abdominal angina, vomiting and dyspepsia associated with weight loss, hence the need of overnight total parenteral nutrition through a central venous catheter. No other medical conditions were reported and all pre-operative laboratory blood tests were normal. Inflammatory bowel diseases and Helicobacter pylori were already ruled out during a previous hospitalization as no response was showed to treatments with high dose proton pump inhibitors and multiple lines of bowel anti-inflammatory drugs.
Under the clinical suspicion of DS, the focused abdominal US exam performed in another Hospital confirmed the MAL syndrome, and 6-month prior the referral to our vascular surgery unit, she underwent surgery with laparoscopic section of the MAL. Few weeks later, she experienced a rapid recurrence of symptoms, so she presented to our Hospital for a new full diagnostic work up.
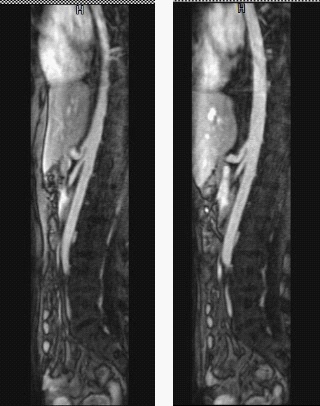
An US Color Doppler exam confirmed the stenosis of the celiac artery (>50%), and the abdomen MRI angiography showed tortuosity of the celiac trunk and dynamic modification of the arterial diameter during deep inspiration and fully forced expiration (Figure 1). Hence, the patient was scheduled for a new laparoscopic procedure to treat the MAL syndrome.
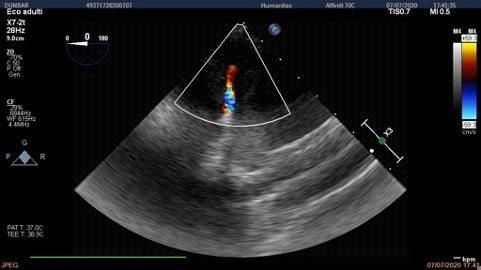
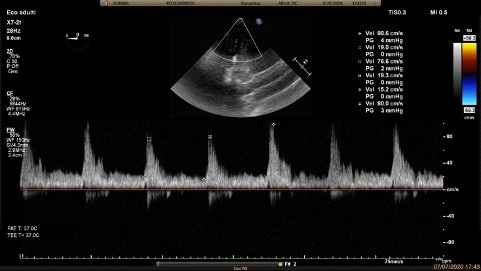
After the induction of general anaesthesia, the transoesophageal echographic transducer was successfully inserted into the patient’s oesophagus. A complete, Systematic Transoesophageal Echocardiography (TEE) was performed, and images were acquired according the guidelines [4]. After cardiac function assessment by upper and mid-esophageal views, the transducer was advanced to the stomach for routine transgastric views, and then it was rotated 180° and flexed posteriorly to locate the descending thoracic aorta. At this level, the color Doppler was used to recognize the celiac trunk (Figure 2) and applying the pulsed wave Doppler we could measure the pick systolic velocity (PSV), resulting 133 cm/s (Figure 3). The correct positioning of the TEE probe was also confirmed by the direct laparoscopic visualization of the shape of the transducer through the stomach wall over the celiac trunk and the MAL.
During the surgery, the TEE probe was left in the same position in standby mode in order not to overheat or damage the gastric mucosa. At the end of the surgical section of the MAL the PSV of the celiac trunk was re-evaluated showing significant drop now oscillating with the respiratory cycle between 76 and 98 cm/s (Figure 4). The patient was then awakened from anaesthesia and after a brief postoperative observation and monitoring, was discharged to the ward. The postoperative period was uneventful, food intake was started the first day after surgery with no pain recurrence, and the patient was discharged from the Hospital on the third postoperative day.

Discussion
In this case of DS we opted to evaluate the celiac artery blood flow by trans-esophageal color-Doppler to obtain a real-time confirmation of the successful surgical correction.
Trans-esophageal Echocardiography (TEE) has been extensively used to evaluate the heart and the thoracic aorta, but there are still few evidences of its usefulness in the evaluation of the superior portion of the abdominal aorta and the celiac trunk [5]. Since trans-gastric visualization of the celiac artery through TEE was proved to be feasible [6], its has been used as an anatomical marker for the orientation on the descending thoracic aorta [7] and a diagnostic tool for the evaluation of aortic dissection [8].
Our patient had already received a surgical treatment for DS, but after that first operation the MAL syndrome re-occurred. Similar outcomes have been described in literature [9]. Hence, we considered that intra-operative evaluation of the surgical efficacy was mandatory in this case. An evaluation of the resection of the MAL could have been obtained by other techniques before and after the operation, but TEE measurement allowed us to do this real-time intra-operatively. Thus, surgeon was assured of the technical success of the operation or conversely he would have been persuaded to change the surgical approach from laparoscopic to a traditional open correction.
Indeed, in our patient the MAL resection was considered successful only after having re-evaluated the celiac artery blood flow velocity and measured its reduction after the correction.
Conclusion
Transoesophageal echocardiography showed to be a practical and reliable tool for the evaluation of the celiac trunk flow alteration due to the Dunbar Syndrome. The intraoperative monitoring of the PSV of celiac artery during the laparoscopic section of the MAL allows the surgeon to confirm the successful outcome of the operation before the awakening of the patient.
References
- Lipshutz B. A Composite Study Of The Coeliac Axis Artery. Ann Surg. 1917; 65: 159-169.
- Kim EN, Lamb K, Relles D, Moudgill N, DiMuzio PJ, Eisenberg JA. Median Arcuate Ligament Syndrome-Review of This Rare Disease. JAMA Surg. 2016; 151: 471-477.
- Tsujimoto H, Hiraki S, Sakamoto N, et al. Laparoscopic treatment for median arcuate ligament syndrome: the usefulness of intraoperative Doppler ultrasound to confirm the decompression of the celiac artery. Surg Laparosc Endosc Percutan Tech. 2012; 22: e71-e75.
- Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: Recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013; 26: 921-964.
- Frazin LJ. Transesophageal echocardiographic detection of thoracic aorta dissection extending into the celiac artery. J Am Soc Echocardiogr. 2003; 16: 1186-1187.
- Frazin LJ, Siddiqui M, Venugopalan K, Pop P, Vonesh MJ, McPherson DD. Feasibility of transcolonic and transgastric abdominal vascular ultrasound. Am J Card Imaging. 1994; 8: 95-99.
- Zhou L, Jariwala N, Frazin L. Should the Celiac Artery Be Used as an Anatomical Marker for the Descending Thoracic Aorta During Transesophageal Echocardiography. Echocardiography. 2016; 33: 66-68.
- López-Pardo F, Gómez-Navarro C, Peiró J, Alcázar M, Villa M, et al. Transesophageal echocardiographic detection of aortic dissection with reentry site at the level of the celiac artery. Echocardiography. 2005; 22: 279-281.
- Klimas A, Lemmer A, Bergert H, Brodhun M, Scholbach T, et al. Laparoscopic treatment of celiac artery compression syndrome in children and adolescents. Vasa. 2015; 44: 305-312.