
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Median arcuate ligament syndrome and liver transplantation
Maitane I Orue-Echebarria1*; Elena Sagarra1; Sergio Carrasco2; Benjamín Díaz-Zorita1
1Transplant and Hepatobiliopancreatic Surgery Unit, Department of General and Digestive Surgery, Hospital General Universitario Gregorio Marañón, Madrid, Spain.
2Department of Radiology, Hospital General Universitario Gregorio Marañón, Madrid, Spain.
*Corresponding Author : Maitane I Orue-Echebarria
General Surgery and Digestive System Service, Hospital General Universitario Gregorio Marañón. c / Doctor Esquerdo 46, 28007, Madrid, Spain.
Email: maoretxe90@hotmail.com
Received : Apr 13, 2021
Accepted : May 10, 2021
Published : May 13, 2021
Archived : www.jcimcr.org
Copyright : © Orue-Echebarria MI (2021).
Keywords: Median arcuate ligament syndrome; liver transplantation; celiac artery; hepatic artery thrombosis.
Citation: Orue-Echebarria MI, Sagarra E, Carrasco S, Díaz-Zorita B. Median arcuate ligament syndrome and liver transplantation. J Clin Images Med Case Rep. 2021; 2(3): 1139.
Background
Arcuate ligament syndrome results from the compression of the celiac artery by the diaphragmatic fibers. It is asymptomatic in most cases and has an incidence of 2 to 24% of the population. In liver transplantation, it has great relevance, since it can be related to various postoperative complications.
Case presentation
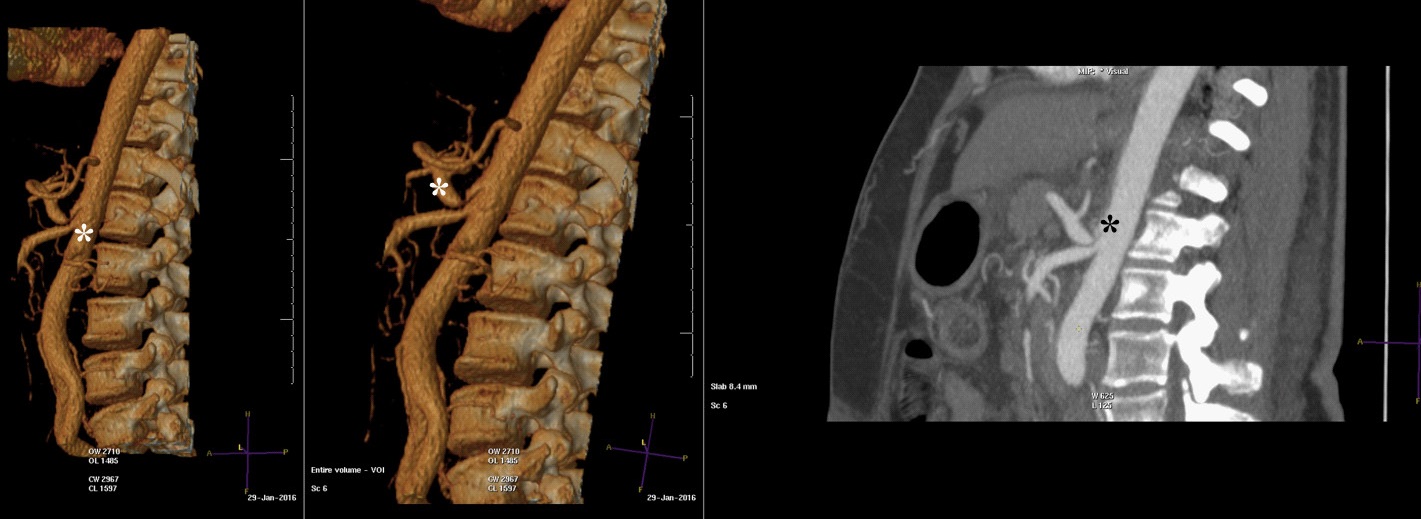
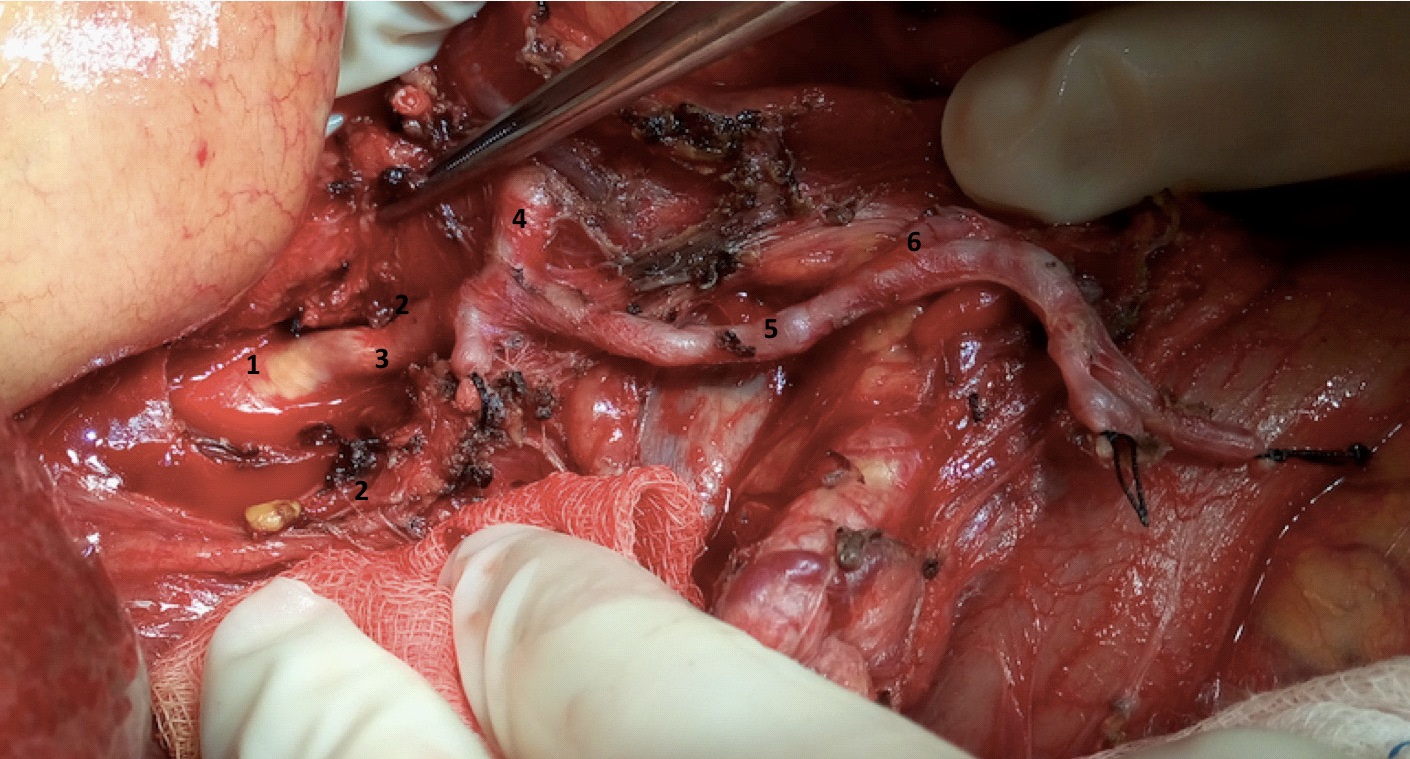
We present the case of a woman who required an urgent hepatic transplant because a fulminant hepatitis by HBV. The arcuate ligament was identified during the pre- transplant tests. Intraoperatively, the release of the arcuate ligament was performed and the implant continued with regularity. The Doppler ultrasound showed good flows and the postoperative period passed without events.
Discussion
The median arcuate ligament causes most of the stenosis of the celiac artery. The flow of organs dependent on the celiac artery is ensured by collaterals. They may be affected during the first phase of orthotopic liver transplantation and as a consequence, compromise the irrigation of the graft, which may lead to failure of the graft. The standard treatment is the release of the celiac artery with the section of the arcuate ligament. The usefulness of this maneuver is verified by checking the flows.
Conclusion
Despite the low incidence of symptomatology in relation to the arcuate ligament syndrome in the general population, its identification and treatment in liver transplantation is imperative since it can lead to graft loss.
References
- Vilatoba M, Zamora-Valdés D, Guerrero-Hernández M, Romero-Talamás H, Leal-Villalpando R, et al. Arcuate ligament compression as a cause of early-onset thrombosis of the hepatic artery after liver transplantation. Ann Hepatol. 2011; 10: 88-92.
- Czigany Z, Boecker J, Morales Santana DA, Bednarsch J, Meister FA, et al. Median Arcuate Ligament Compression in Orthotopic Liver Transplantation: Results from a Single-Center Analysis and a European Survey Study. J Clin Med. 2019; 8: 550.
- Jiang ZJ, Liang TB, Feng XN, Wang WL, Shen Y, et al. Arcuate ligament syndrome inducing hepatic artery thrombosis after liver transplantation. Hepatobiliary Pancreat Dis Int. 2008; 7: 433-436.
- Lubrano J, Scatton O, Randone B, Molinier N, Massault P, et al. Median Arcuate Ligament in Orthotopic Liver Transplantation: Relevance to Arterial Reconstruction. Trans Proceed 2008; 40: 3532–3535.