
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Successful repair of an anomalous right coronary artery arising from the pulmonary artery in a 10 month-old
Matthew C Schwartz1*; William Hammill2; Thomas S Maxey3
1Division of Pediatric Cardiology, Sanger Heart and Vascular Institute, Charlotte, NC, USA.
2Division of Pediatric Cardiology, Novant Health, Charlotte, NC, USA.
3Division of Pediatric Cardiac Surgery, Sanger Heart and Vascular Institute, Charlotte, NC, USA.
*Corresponding Author : Matthew C Schwartz
Atrium Health, Sanger Heart and Vascular Institute, Levine Children’s Hospital, 1001 Blythe Blvd, Suite 200D, Charlotte, NC 28203, USA.
Email: Matthew.c.schwartz@atriumhealth.org
Received : Apr 14, 2021
Accepted : May 10, 2021
Published : May 13, 2021
Archived : www.jcimcr.org
Copyright : © Schwartz MC (2021).
Citation: Schwartz MC, Hammill W, Maxey TS. Successful repair of an anomalous right coronary artery arising from the pulmonary artery in a 10 month-old. J Clin Images Med Case Rep. 2021; 2(3): 1140.
Case report
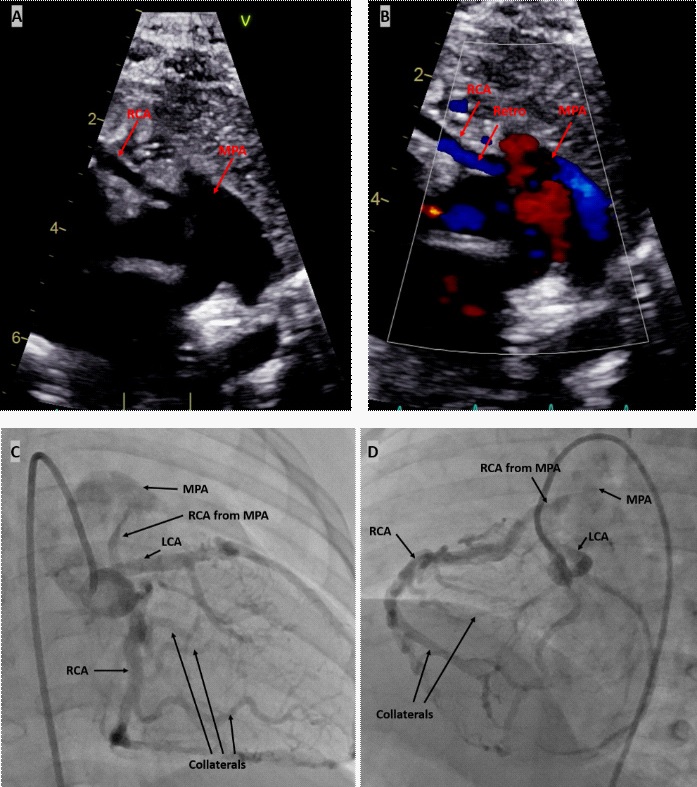
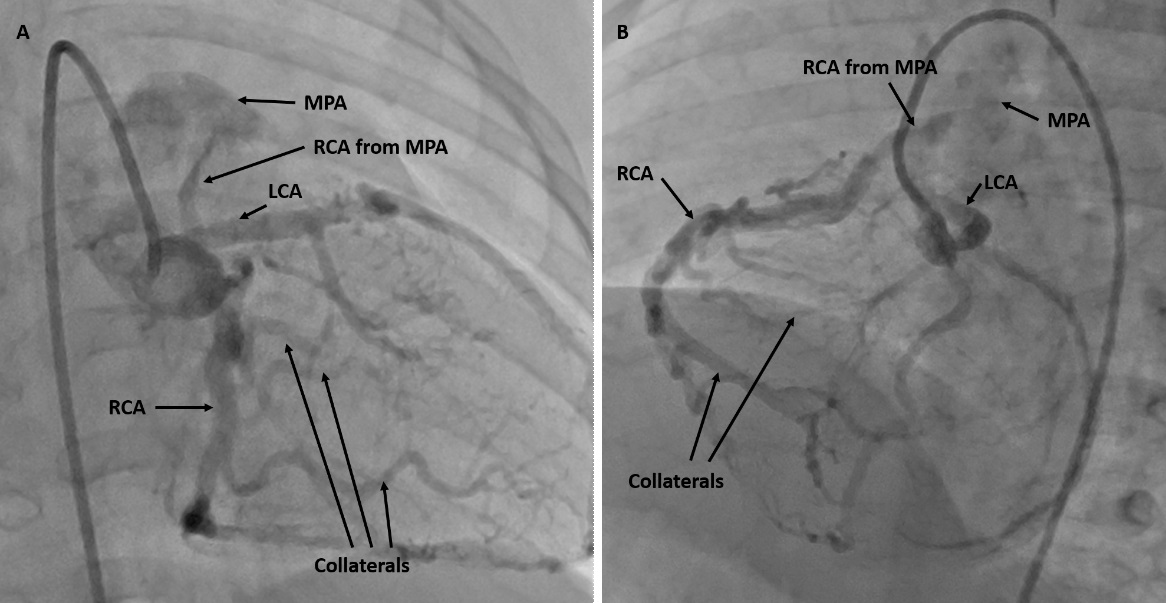
Echocardiogram (Figure 1A-B) in an asymptomatic 6 month-old raised suspicion for anomalous Right Coronary Artery (RCA) from the Pulmonary Artery (ARCAPA) with retrograde flow from the RCA to the main pulmonary artery. The patient’s left ventricular systolic function was normal. Subsequent cardiac catheterization confirmed the diagnosis as angiography showed that the RCA arose from the anterior aspect of the main pulmonary artery and filled retrograde via a collateral network from the Left Coronary Artery (LCA) system (Figure 1C-D). At 10 months of age, the patient underwent surgical translocation of the RCA to the aorta. On direct visualization, the RCA arose from the anterior wall of the main pulmonary artery and the robust collateral supply of the RCA from the LCA was visualized on the heart’s epicardium (Figure 2). The patient did well and was discharged home several days later. Three months after the operation, the patient continues to do well with normal left ventricular systolic flow and prograde flow into the reimplanted RCA.
Discussion
ARCAPA is a rare congenital coronary anomaly, occurring in 0.002% of the population. It is less common than anomalous left coronary artery from the pulmonary artery (ALCAPA) which occurs in 0.008% of the population. In patient’s with ALCAPA, as the pulmonary vascular resistance and pulmonary artery pressure decrease over the first 2 months of life, the coronary perfusion pressure to the left coronary system decreases. Collateral supply from the RCA to the lower pressure left coronary artery system can develop, but myocardial perfusion to the high-pressure, thick-walled left ventricle is commonly compromised. Many patients present in infancy with severely decreased left ventricular systolic function due to myocardial infarction [1].
In contrast, the clinical course associated with ARCAPA is less severe. Diagnosis is rare in young children as most are asymptomatic [2,3]. It is hypothesized that infarction is less likely to develop because the RCA supplies a smaller amount of myocardium compared to the LCA and because much of the RCA distribution supports the lower pressure right ventricle with decreased oxygen demand [1]. Nonetheless, infarction and sudden death have been reported early in childhood [1]. In addition, 40% of patients with ARCAPA have additional forms of congenital heart disease and it most commonly occurs concominant with an aortopulmonary window or tetralogy of Fallot [3].
Because infarction and sudden death may occur, corrective operation is recommended even in the absence of symptoms or myocardial dysfunction. Reimplantation of the RCA is the preferred intervention, although rare reports of RCA ligation exist [1]. Ligation of the RCA is not ideal as the patient is left with a single ostium coronary arterial system which may be associated with higher risk of infarction and sudden death. After antegrade flow from the aorta to the RCA is established, the LCA system normalizes in size [4]. Most do well after RCA reimplantation, but there are few reports of long-term follow up after this operation [1,3]. Late complications after reimplantation of the RCA have been described including RCA thrombosis and stenosis [1,2]. Thus, continued surveillance after repair is warranted.
References
- Williams IA, Gersony WM, Hellenbrand WE. Anomalous right coronary artery arising from the pulmonary artery: A report of 7 cases and a review of the literature. American heart journal. 2006; 152: e9-17.
- Grabowski K, Karolczak MA, Zacharska-Kokot E, et al. Anomalous origin of the right coronary artery from the main pulmonary artery treated surgically in a 6-week-old infant. A case report and review of the literature. Journal of ultrasonography. 2018; 18: 71-76.
- Radke PW, Messmer BJ, Haager PK, et al. Anomalous origin of the right coronary artery: preoperative and postoperative hemodynamics. The Annals of thoracic surgery. 1998; 66: 1444-1449.
- van Meurs-van Woezik H, Serruys PW, Reiber JH, et al. Coronary artery changes 3 years after reimplantation of an anomalous right coronary artery. European heart journal. 1984; 5: 175-178.