
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Acute cardiotoxicity after initiation of the novel tyrosine kinase inhibitor gilteritinib for acute myeloid leukemia
Lisa Kim1; Brian Fowler1; Jeremy Slivnick1; Haseeb Nawaz1; Yaquta Kaka1; Patrick Ruz1; Ajay Vallakati1; Ragavendra Baliga1; Sumithira Vasu2; Daniel Addison1,3*
1Cardio-Oncology Program, Division of Cardiology, Department of Internal Medicine, The Ohio State University Medical Center, Columbus, OH, USA.
2Bone Marrow Transplantation and Cellular Therapies Program, Division of Hematology, The Ohio State University James Comprehensive Cancer Center, Columbus, OH, USA.
3Division of Cancer Control and Prevention, James Cancer Hospital and Solove Research Institute at The Ohio State University, Columbus, Ohio, USA.
*Corresponding Author : Daniel Addison
Division of Cardiology, The Ohio State University Wexner Medical Center, Davis Heart and Lung Research Institute, 473 W. 12th Ave. Columbus, OH, 43210, USA
Email: [email protected]
Received : Apr 14, 2021
Accepted : May 10, 2021
Published : May 13, 2021
Archived : www.jcimcr.org
Copyright : © Addison D (2021).
Abstract
Gilteritinib is a novel tyrosine kinase inhibitor recently approved by the United States Food and Drug Administration in 2018 for relapsed or refractory Acute Myeloid Leukemia (AML). However, gilteritinib may be associated with previously underrecognized cardiotoxicities. This case describes a patient without prior cardiovascular history who was diagnosed with relapsed AML. After six doses of gilteritinib initiation, she abruptly developed acute systolic heart failure with global hypokinesis and septal wall motion abnormalities. Two days after discontinuation, cardiac Magnetic Resonance Imaging (MRI) showed recovery of her Left Ventricular Ejection Fraction (LVEF) as well as myocardial edema and non-ischemic fibrosis suggestive of inflammatory cardiomyopathy. She was started on guideline directed heart failure therapy. Follow up cardiac MRI five months later showed recovery of LVEF with mild non-ischemic fibrosis and resolution of myocardial edema and inflammation. She later received an allogeneic stem cell transplant from a matched unrelated donor.
Keywords: Gilteritinib; FLT3-mutation; Cardio-oncology; Acute myeloid leukemia; Cardiac MRI.
Abbreviations: TKI: Tyrosine Kinase Inhibitor; FLT3: FMS-Like Tyrosine Kinase 3; AML: Acute Myeloid Leukemia; ECG: Electrocardiogram; TTE: Transthoracic Echocardiogram; LVEF: Left Ventricular Ejection Fraction; MRI: Magnetic Resonance Imaging.
Citation: Addison D, Kim L, Fowler B, Slivnick J, Nawaz H, et al. Acute cardiotoxicity after initiation of the novel tyrosine kinase inhibitor gilteritinib for acute myeloid leukemia. J Clin Images Med Case Rep. 2021; 2(3): 1141.
Introduction
Constitutive activation of FMS-like tyrosine kinase 3 (FLT3) occurs in approximately 30% of Acute Myeloid Leukemias (AML) and is clinically associated with an aggressive disease course with higher rates of relapse [1,2]. FLT3 inhibitors have shown promising antileukemic activity in recent clinical trials. Gilteritinib, a novel tyrosine kinase inhibitor of FLT3, was rapidly approved by the United States Food and Drug Administration (FDA) in 2018 after the multicenter, randomized phase III ADMIRAL trial, which demonstrated significantly higher overall survival and response rates in comparison with salvage chemotherapy in AML. This trial established gilteritinib monotherapy as the new standard for relapsed or refractory FLT3-mutated AML [2]. However, gilteritinib may be associated with previously unrecognized cardiotoxicities. Here, we present a case of acute heart failure and evidence of drug-induced myocarditis in a patient with relapsed AML treated with gilteritinib, which improved upon withholding therapy. We also review other potential cardiac toxicities linked with this emerging drug class.
Case presentation
A 56-year-old woman with a history of hyperlipidemia and AML in complete remission after 7 + 3 induction chemotherapy with cytarabine and daunorubicin followed by maintenance therapy with azacitadine presented to the emergency department with recurrent fevers to 102°F, generalized myalgias, fatigue, pharyngitis and diffuse bruising. Examination was notable for oropharyngeal exudates, cervical lymphadenopathy and generalized ecchymosis on all extremities. She was found to have new leukocytosis to 53 K/uL with 86% circulating blasts, acute anemia to 7 g/dL and new thrombocytopenia to 18 K/uL, concerning for AML recurrence. She underwent empiric treatment for febrile neutropenia. Computed tomography of the chest revealed patchy nodular opacities in the mid to lower lungs with ground glass airspace disease. Broad immunocompromised infectious workup was unremarkable for bacterial, viral and fungal infections. She eventually underwent bronchoscopy and was subsequently diagnosed with Serratia marcescens pneumonia for which she received empiric treatment. Mutational analysis of her peripheral blood revealed new FLT3 internal tandem duplications (FLT3-ITD) as an attractive therapeutic target for relapsed AML. She underwent cytoreductive therapy with hydroxyurea before transitioning to single agent FLT3 targeted therapy with gilteritinib as standard of care. Prior to initiating targeted therapy, baseline Electrocardiogram (ECG) and Transthoracic Echocardiogram (TTE) were unremarkable with Left Ventricular Ejection Fraction (LVEF) of 67%.
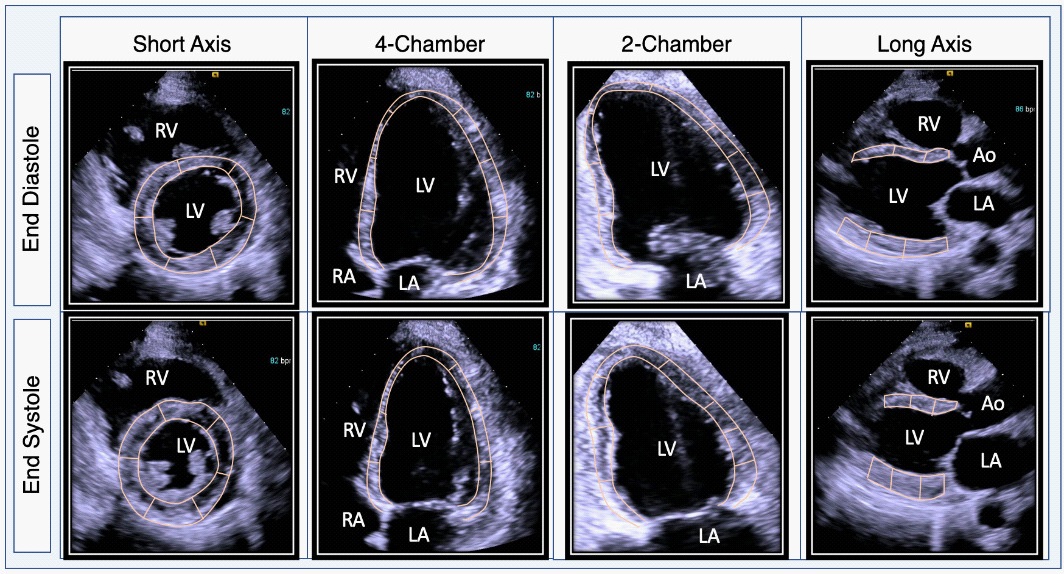
Following just six doses of gilteritinib, the patient developed worsening shortness of breath, orthopnea, paroxysmal nocturnal dyspnea, bilateral lower extremity edema and 23-pound weight gain. Examination was notable for new jugular venous distension, bibasilar crackles and abdominal distension with 2+ pitting edema. Gilteritinib was promptly discontinued due to concern for acute cardiotoxicity and the patient progressed to acute hypoxic respiratory failure requiring 8 liters of supplemental oxygen. Brain natriuretic peptide was elevated to 1,574 pg/mL (from 195 pg/mL five days prior, normal <100 pg/mL) and troponin to 36 ng/mL (normal <11 ng/mL). ECG did not reveal ischemic changes and chest radiography revealed new cardiomegaly and worsening bilateral airspace disease. Repeat TTE ruled out pericardial effusion but demonstrated newly reduced LVEF to 36% from 67% five days prior, now with focal septal hypokinesis, new moderate to severe tricuspid regurgitation and elevation of right ventricular systolic pressure to 50 mm Hg (Figure 1). Cardiac magnetic resonance imaging (MRI) obtained two days after discontinuation of gilteritinib revealed borderline biventricular function with interval improvement in LVEF to 51%. Late-gadolinium enhancement imaging revealed patchy midwall fibrosis involving the septal and lateral walls and elevated T2 signal in the inferoseptum (up to 70 ms; normal <53 ms) suggestive of myocardial edema or inflammation, findings which were consistent with an inflammatory cardiomyopathy (Figure 2).
In the absence of alternative explanations, gilteritinib associated acute systolic heart failure and inflammatory cardiomyopathy was considered the most probable etiology given the timeline of symptoms. Gilteritinib was promptly discontinued. During this time, she underwent intravenous diuresis with furosemide and started guideline directed medical therapy for non-ischemic cardiomyopathy with metoprolol succinate, lisinopril and spironolactone. Subsequent TTE three months later showed improvement of left ventricular function to 45-50% with mild global hypokinesis. Follow up cardiac MRI five months later showed recovered LV function with mild non-ischemic fibrosis and resolution of myocardial edema and inflammation on T2 mapping compared to prior (Figure 2). The patient subsequently received two cycles of azacitidine and venetoclax before achieving morphologic and molecular remission of AML confirmed by bone marrow biopsy. She went on to receive an allogeneic stem cell transplant from a matched unrelated donor.

Discussion
To our knowledge, this is the first reported case of acute systolic heart failure associated with gilteritinib therapy in a patient without pre-existing cardiovascular disease. Baseline cardiac screening prior to treatment initiation did not reveal subclinical cardiomyopathy. After six doses of gilteritinib therapy, this patient abruptly developed symptoms of new onset heart failure with an acute reduction in LVEF to 37%. Further diagnostic evaluation with cardiac MRI showed mid wall myocardial edema on T2-weighted imaging and late gadolinium enhancement in a non-coronary artery distribution, suggestive of myocarditis. Definitive diagnosis with endomyocardial biopsy was deferred due to its associated procedural risks and low likelihood of altering management. Due to a lack of alternative explanations, acute systolic heart failure due to gilteritinib therapy was determined to be the most probable cause. Notably, rapid reversibility of cardiac dysfunction was observed within two days upon discontinuation of gilteritinib. This patient eventually recovered from symptomatic heart failure with stable LVEF after cessation of targeted therapy and introduction of guideline directed heart failure therapy. She was able to successfully receive further cancer treatment.
In general, the onset, timeline and likelihood of recovery from early cardiotoxicities associated with FLT3 inhibitors is unclear. There is increasing evidence that FLT3 tyrosine kinase inhibitors are associated with cardiotoxicities, such as cardiomyopathies and QT prolongation [3]. However, the incidence of adverse cardiovascular events associated with emerging targeted therapies has not been fully characterized. Currently, the FDA approved two FLT3 inhibitors, gilteritinib and midostaurin, for FLT3 mutated AML [2,4,5]. Gilteritinib gained approval after the phase III ADMIRAL trial, which demonstrated significantly higher overall survival (9.3 months vs 5.6 months) and response rates (34% vs 15.3%) in comparison with salvage chemotherapy in relapsed or refractory AML [2]. However, clinically significant adverse cardiovascular events were also observed among 138 enrollees within the first 30 days of therapy, including QT prolongation (7%), cardiac failure (4%), pericardial effusion (4%), pericarditis and myocarditis (2%) [4]. Similarly, midostaurin, a multi-kinase FLT3 inhibitor approved for combination with induction chemotherapy for newly diagnosed FLT3 mutated AML, was associated with significant cardiotoxicities such as QT prolongation, leading to dose modification or treatment discontinuation [5]. Other adverse cardiac events in <10% of patients included cardiac failure (6%), myocardial infarction or ischemia (4%), and QT prolongation [5]. With real world clinical use, cardiotoxicities associated with emerging FLT3 inhibitors have become increasingly evident and may present unique clinical challenges regarding oncologic treatment decisions [3].
A mechanistic explanation of gilteritinib associated cardiotoxicity is currently limited as the functional role of FLT3 signaling in cardiomyocytes is incompletely understood. Pfister et al. explored the role of FLT3 and FLT3 ligand signaling in the heart and proposed that activation of FLT3 signaling may serve as a cardioprotective anti-apoptotic system in the setting of oxidative stress and myocardial injury. They speculate that off target inhibition of FLT3 signaling in antileukemic targeted therapies may result in loss of this cardioprotective mechanism and lead to cardiomyocyte death, which may be a potential explanation for cardiotoxicity seen in FLT3 targeted cancer therapies [6]. Although the exact mechanism remains unclear, tyrosine kinase FLT3 inhibitors have been associated with significant cardiotoxicities, which is an important limitation in cancer therapy [3].
Currently, multiple clinical trials are exploring the role of gilteritinib in combination regimens [7]. However, observed cardiovascular event rates used to guide most cardiotoxicity risk assessments in pivotal cancer clinical trials and during years of cumulative follow up have been underreported [3,8]. Moving forward, baseline and ongoing cardiovascular surveillance, even in patients without cardiovascular disease, is particularly important for monitoring early and late cardiotoxicity
Conclusion
This case demonstrates the potential for developing acute systolic heart failure, inflammatory cardiomyopathy and possible myocarditis with novel tyrosine kinase inhibitors, such as gilteritinib, even in patients without pre-existing cardiovascular disease. The timeline and likelihood of reversibility of cardiac dysfunction from FLT3 inhibition remains unclear. Clinicians are advised to obtain baseline and ongoing cardiovascular assessment in patients on targeted therapies for early recognition of potentially serious but rare cardiovascular complications of gilteritinib therapy.
Funding: This work was supported, in part, by National Cancer Institutes (NCI) grants: P30 CA016058, and K12CA133250 (Dr. Addison).
Disclosures: All authors declare no conflicts of interests in relation to the work presented in this manuscript.
References
- Perl AE, Martinelli G, Cortes JE et al. Gilteritinib or Chemotherapy for Relapsed or Refractory. N Engl J Med. 2019; 381: 1728-1740.
- Megías-Vericat JE, Martínez-Cuadrón D, Sanz M, Montesinos P. Salvage regimens using conventional chemotherapy agents for relapsed/refractory adult AML patients: A systematic literature review. Ann Hematol. 2018; 97: 1115-1153.
- Gronich N, Lavi I, Barnett-Griness O, Saliba W, Abernethy DR, et al. Tyrosine kinase-targeting drugs-associated heart failure. Br J Cancer. 2017; 116: 1366-1373.
- Astellas Pharma. XOSPATA® (gilteritinib): US Prescribing Information. 2018.
- Novartis Pharma. RYDAPT® (midostaurin): US Prescribing Information. 2017.
- Pfister O, Lorenz V, Oikonomopoulos A et al. FLT3 activation improves post-myocardial infarction remodeling involving a cytoprotective effect on cardiomyocytes. J Am Coll Cardiol. 2014; 63: 1011-1019.
- Zhao J, Song Y, Liu D. Gilteritinib: A novel FLT3 inhibitor for acute myeloid leukemia. Biomark Res. 2019; 7: 19.
- Bonsu JM, Guha A, Charles L et al. Reporting of Cardiovascular Events in Clinical Trials Supporting FDA Approval of Contemporary Cancer Therapies. J Am Coll Cardiol. 2020; 75: 620-628.