
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Cecal herniation through the foramen of winslow: Case presentation and literature review
Jena Deitrick; William Sessions; Daniel Nguyen; Ariel Santos*
School of Medicine TTUHSC @ Amarillo, Texas, USA.
*Corresponding Author : Ariel Santos
School of Medicine TTUHSC @ Amarillo, 3601 4th Street, STOP Mail 7563, Lubbock, TX 79430, USA.
Email: ariel.santos@ttuhsc.edu
Received : Apr 15, 2021
Accepted : May 11, 2021
Published : May 14, 2021
Archived : www.jcimcr.org
Copyright : © Santos A (2021).
Abstract
Foramen of Winslow hernias are a rare type of internal hernia that account for less than 1% of all cases of intestinal obstruction. It is extremely rare surgical condition with estimated mortality of about 50%. Timely diagnosis aided by computed tomography (CT scan) can facilitate proper planning and surgical treatment. Optimal treatment depends on patient’s condition, status of the incarcerated structure as well as surgeon’s comfort and preference.
Citation: Deitrick J, Sessions W, Nguyen D, Santos A. Cecal herniation through the foramen of winslow: Case presentation and literature review. J Clin Images Med Case Rep. 2021; 2(3): 1144.
Introduction
Internal hernias are relatively rare causes (0.5-6% of all cases) of intestinal obstruction [1,2]. Of these, only 8% involve herniation through the Foramen of Winslow, the passageway between the greater sac and the lesser sac [2]. Since this condition is very uncommon, there is often a delayed or even a missed diagnosis. For this reason, it was once estimated to have a mortality of up to 49% [3]. Improvements in radiologic imaging and increased awareness can aid in establishing diagnosis and surgical intervention to produce improved outcomes for affected patients. As this condition is more routinely diagnosed pre-operatively, some clinicians beg the question whether an open or laparoscopic approach lends to improved outcome and speculate about how to prevent recurrence.
Case presentation
A 53-year-old lady presented to the emergency department with episodic sharp epigastric and periumbilical pain that radiated diffusely throughout her entire abdomen. Patient denied nausea, vomiting, diarrhea, constipation, fever, or chills, and she reported passing both gas and stool one day prior to admission. Past medical history included hyperlipidemia and hypothyroidism, which were both adequately treated. She denied any past surgical history. Physical examination revealed a distended abdomen which is tender upon palpation at the epigastric region with guarding. The remainder of the physical examination and all vital signs were within normal limits.
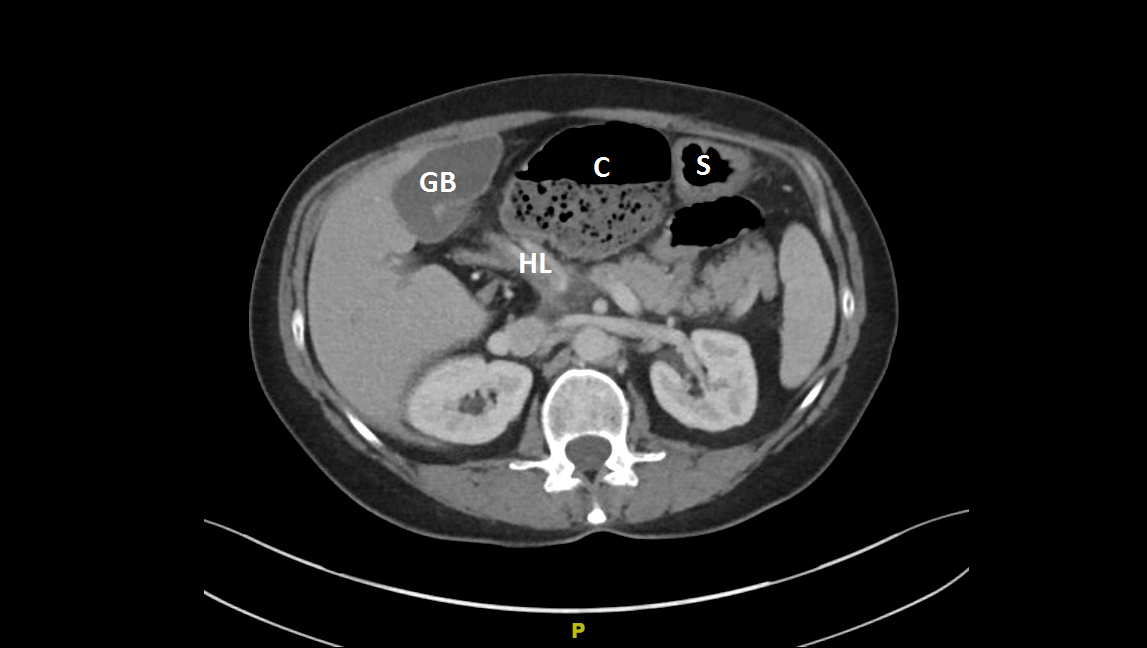
Computed Tomography (CT) of the abdomen was requested (Figure 1-3) which revealed: Malposition of the cecum and ascending colon, swirling and edematous changes of the mesentery, dilatation of the cecum and ascending colon with focal narrowing of the rest of the large bowel, and free fluid within the posterior aspect of the pelvis. The liver, gallbladder, pancreas, and spleen appeared normal, and there was no intraperitoneal free air. There was normal enhancement of the kidneys, mild bilateral hydronephrosis, and mild diffuse thickening of the bladder wall. The overall radiologic impression was consistent with cecal volvulus. Secondary to the patient’s clinical examination findings and the radiological image concerning for cecal volvulus, the decision was made to proceed with open abdominal surgical exploration.
The patient was admitted and started on intravenous antibiotics and aggressive fluid resuscitation. Surgical exploration via midline laparotomy revealed that the patient’s terminal ileum and cecum had herniated through the foramen of Winslow into the lesser sac. Furthermore, the herniated cecum had rotated inside the lesser sac, resulting in volvulus and massive cecal dilatation. Reduction of the viable herniated cecum was unsuccessful. We proceeded with right hemicolectomy with side-to side ileo-colonic stapled anastomosis. In addition, cholecystectomy was performed due to evidence of acute cholecystitis.


Discussion
Intestinal herniation through the Foramen of Winslow is a rare presentation; only about 200 cases have been reported since its initial description in 1834 [4]. Due to its rarity and vague symptoms, the diagnosis is often missed or not made until surgical exploration is performed. Widespread use of Computed Tomography (CT) and increased awareness of this and other internal hernias as a cause of intestinal obstruction have led to increased pre-operative diagnosis and accelerated treatment, which has allowed for decreased mortality associated with the condition. Historically, the associated mortality approached 50%, but more recent reports indicate a mortality of only 5% [5]. Intestinal herniation through the Foramen of Winslow presents with vague symptoms of intestinal obstruction, such as colicky abdominal pain, nausea, vomiting, abdominal distension, and constipation [2-12]. Due to its location adjacent to the hepatoduodenal ligament, jaundice can also occur if the hernia compresses the common bile duct [2]. It has also reportedly caused gastric outlet obstruction in a few cases [6]. Since the presentation is very nonspecific, it may be mistaken for appendicitis, gastroenteritis, ectopic pregnancy, ovarian torsion, rupture of ovarian cyst, cholecystitis, cholelithiasis, or other causes of intestinal obstruction. One specific aspect of the presentation is relief of pain by complete truncal flexion (knees to chest position); this position alleviates pain by opening the Foramen of Winslow and decreasing tension on the incarcerated bowel [3,8]. However, not every patient reports this alleviating factor, and imaging is often required to make the diagnosis.
While some report signs of Foramen of Winslow herniation on plain X-rays, CT scan is critical in the pre-operative diagnosis. Common findings on CT include: Dilated non-encapsulated fluid-filled bowel loops in the lesser sac anterior to the inferior vena cava, stomach/pancreas/spleen displaced anteriorly or laterally, engorged and stretched out mesenteric vessels, absence of ascending colon in the right paracolic gutter, and displacement of the first and second portions of the duodenum to the left [1,13,14]. The increased use of CT has increased pre-operative diagnosis from 10% to about 86% in recent years. Despite these great improvements made possible by CT, Foramen of Winslow hernias are still misdiagnosed as other conditions, including cecal volvulus [3]. In retrospect, the original CT scans of our patient (Figure 1-3) showed signs of cecal herniation through the Foramen of Winslow, including lateral displacement of the stomach and compression of the vessels encased by the hepatoduodenal ligament. Some experts assert that when the CT impressions are not definitive, multidetector computed tomography (MDCT) can aid in diagnosis [1]. Increased awareness of these specific CT findings will lead to quicker and more accurate diagnosis of these rare internal hernias. It is imperative for clinicians to review radiographic images rather than relying on radiologist’s report. Taking time to discuss the salient radiographic signs as it correlates with the patient’s symptoms can expedite diagnosis and facilitate appropriate treatment.
As the shift from intra-operative to pre-operative diagnosis of Foramen of Winslow hernias occurs, it leads to the discussion of whether an open or laparoscopic approach results in better outcomes. The first laparoscopic repair of a Foramen of Winslow hernia occurred in 2011, and a few other have followed [4,5,8,11]. All of them were successful, and one even demonstrated the ability to decompress distended herniated bowel laparoscopically. However, none of these cases required resection of unviable bowel, so this may be a limitation to the utility of a laparoscopic approach. As the laparoscopic approach gains favor in other more common surgical procedures, we expect internal hernia repairs to follow this trend. The surgical management of cecal herniation through Foramen of Winslow hinged on the patient’s overall condition, if she can tolerate abdominal insufflation during laparoscopic surgery as well as the surgeon’s preference and comfort level. In addition, after the reduction of incarcerated cecum and possibly resecting the herniated bowel, many surgeons have performed additional procedures to prevent recurrence, including right colonic fixation, cecopexy, right hemicolectomy, and closure of the Foramen of Winslow [5-7,10,11].
Conclusion
While intestinal herniation through the Foramen of Winslow is extremely rare, it is imperative to increase awareness of the clinical and radiologic findings associated with this condition to aid in appropriate pre-operative diagnosis, surgical planning and treatment. It is imperative for clinicians to review radiographic images, discuss the images with radiologist and not rely on the readings alone. Furthermore, additional discussion is required to determine the optimal surgical technique (open versus laparoscopic) and interventions to prevent recurrence.
References
- Murali AR, Uma D, Bhawna D, et al. Internal hernias: Surgeons dilemma-unravelled by imaging. Indian J Surg. 2014; 76: 323–28.
- Salar O, El-Sharkawy AM, Singh R, et al. Internal hernias: A brief review. Hernia. 2013; 17: 373–377.
- Powell-Brett SF, Royle JT, Stone T, et al. Caecum herniation through the Foramen of Winslow. JSCR. 2012; 12:1-3.
- Duinhouwer L, Deerenberg E, Rociu E, et al. Herniation of the colon through the Foramen of Winslow: A Case Report. International Journal of Surgery Case Reports. 2016; 24: 14–17.
- Daher R, Montana L, Abdullah J, et al. Laparoscopic management of Foramen of Winslow incarcerated hernia. Surgical Case Reports. 2016; 2.
- Hayes L, Newton C. Gastric Outlet Obstruction Secondary to Caecal Herniation into the Lesser Sac. JSCR. 2017; 4.
- Sikiminywa-Kambale P, Anaye A, Roulet D, et al. Internal Hernia through the Foramen of Winslow: A diagnosis to consider in moderate epigastric pain. JSCR. 2014; 6.
- Ryan J, Jin S, Frank J, et al. Internal Herniation of the Caecum through the Foramen of Winslow: Images for Surgeons. ANZ J SURG. 2014; 4: 95–96.
- Leung E, Bramhall S, Kumar P, et al. Internal Herniation through Foramen of Winslow: A Diagnosis Not to Be Missed. Clinical Medicine Insights: Gastroenterology. 2016; 9: 31-33.
- Osvaldt AB, Mossmann DF, Bersch VP, et al. Intestinal Obstruction Caused by a Foramen of Winslow Hernia. Am J of Surg. 2008; 196: 242–244.
- Garg S, Flumeri-Perez G, Perveen S, et al. Laparoscopic repair of Foramen of Winslow hernia. Int J Angiol. 2015; 25: 064–067.
- Cho H and Kang J. Spontaneous reduction of small bowel herniation through the Foramen of Winslow: Importance of a timely approach. Ann Surg Treat Res. 2017; 92: 113-116.
- Selçuk D, Kantarci F, Oğüt G, et al. Radiological evaluation of internal abdominal hernias. Turk J Gastroenterol. 2005; 16: 57–64.
- Martin L, Merkle E, and Thompson W. Review of internal hernias: Radiographic and clinical findings AJR. 2006; 186: 703–717.