
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Stenosing colon neoplasia causing colonic perforation in a patient with morgagni-larrey’s hernia
María del Pilar Gutiérrez Delgado*; Laura Romacho López; Santiago Mera Velasco; Pablo Fernández Galeano; Julio Santoyo Santoyo
Regional University Hospital of Malaga, Malaga, Spain.
*Corresponding Author : María del Pilar Gutiérrez Delgado
Regional University Hospital of Malaga, Malaga, Spain.
Email: pilargutierrezdelgado@gmail.com
Received : Apr 15, 2021
Accepted : May 11, 2021
Published : May 14, 2021
Archived : www.jcimcr.org
Copyright : © Delgado MDPG (2021).
Citation: Delgado MDPG, López LR, Velasco SM, Galeano PF; Santoyo JS. Stenosing colon neoplasia causing colonic perforation in a patient with morgagni-larrey’s hernia. J Clin Images Med Case Rep. 2021; 2(3): 1147.
Introduction
Congenital diaphragmatic hernia, is a congenital abnormality, rare in adults with a frequency of 0.17-6%.
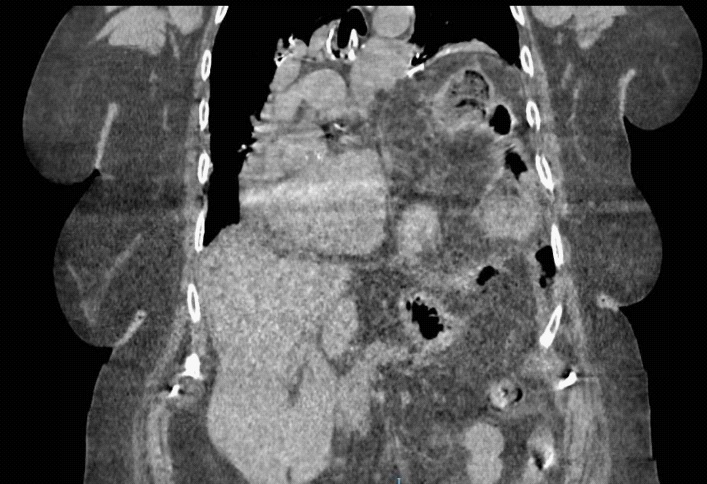
We present the case of an 88-year-old female patient with a history of arterial hypertension, obesity and bronchial asthma. She attended the emergency department of our center with diffuse abdominal pain associated with vomiting, absence of intestinal transit for 4 days and respiratory distress. Laboratory tests showed 11750 leukocytes/μl and PCR 127 mg/L. On suspicion of acute abdomen, a Computerized Tomography (CT) scan was performed (Figure 1), showing a left Morgagni-Larrey Hernia (MH) with gastric chamber and colon inside, with abundant pneumoperitoneum. At surgery we found there was a diffuse purulent peritonitis due to perforation of the transverse colon, which, like the gastric chamber and spleen, was located within a large left diaphragmatic hernia. An extended right hemicolectomy until the tumor in the splenic angle of the colon was surpassed was performed.
Congenital diaphragmatic hernia, is a congenital abnormality, rare in adults with a frequency of 0.17-6% [1]. Morgagni hernia was first described in 1769 by the Italian anatomist Giovanni Battista Morgagni as an anterior diaphragmatic hernia. The most common contents of the hernia sac include the omentum, colon, small bowel, stomach, and portions of the liver. MH can occur on each side of the sternum; however, it is more common on the right side. Most cases are asymptomatic. There are no guidelines for surgical treatment, owing to the rarity of cases, however, surgical repair is indicated in all cases to prevent strangulation [2].
We present the case of an 88-year-old female patient with a history of arterial hypertension, obesity and bronchial asthma. She attended the emergency department of our center with diffuse abdominal pain associated with vomiting, absence of intestinal transit for 4 days and respiratory distress. On examination, the patient had a tendency to arterial hypotension, respiratory distress and desaturation requiring oxygen therapy, a distended and tympanic abdomen, painful on diffuse palpation with peritoneal irritation in the upper hemiabdomen. Laboratory tests showed 11750 leukocytes/μl and PCR 127 mg/L. On suspicion of acute abdomen, a Computerized Tomography (CT) scan was performed (Figure 1), showing a left Morgagni-Larrey Hernia (MH) with gastric chamber and colon inside, with abundant pneumoperitoneum of probable origin in the gastric chamber. Due to the patient’s clinical situation and the radiological findings, urgent surgery was decided.
During surgery, there was evidence of diffuse purulent peritonitis due to perforation of the transverse colon, which, like the gastric chamber and spleen, was located within a large left diaphragmatic hernia. During the exploration of the intestinal package, stenosing neoplasia of the colon at the level of the splenic angle was found, causing retrograde dilatation of the proximal colon and its subsequent perforation. A reduction of the hernial sac content was performed, as well as an extended right hemicolectomy until the tumor in the splenic angle of the colon was surpassed (Figure 2). Due to the patient's hemodynamic instability throughout the surgical procedure, it was decided to place an open abdomen system with negative pressure for surgical revision in 24-48 hours in order to optimize the patient's hemodynamics. After the operation, she was transferred to the Intensive Care Unit, where, despite vasoactive drugs and fluid therapy, the patient died 12 hours after the operation due to multi-organ failure.
The case is striking because of the combination of an important left diaphragmatic defect with a colon perforation and a stenosing colon neoplasia. We are not aware of another such case in the English-language literature. Our patient’s symptoms, and trajectory towards retrograde dilatation of colon due to stenosing colon neoplasia and posterior colon perforation within the hernia, supports the existing teaching that maybe there is no role for watchful waiting in the case of Morgagni hernia. Surgical repair of Morgagni hernia is indicated in all patients to avoid morbidity due to incarceration or ischemic changes of abdominal contents in the chest [3].
The defect is congenital, though trauma or factors which raise intra-abdominal pressure such as obesity, pregnancy, chronic asthma, are implicated in hernia formation [1-4]. Approaches for repair can be abdominal or thoracic (specially for patients who have undergone previous abdominal operation) [4]. Minimally invasive treatment may eventually replace laparotomy approach, however, for this condition is technically challenging [3,4]. In our patient, based on hemodynamic situation we decided to practice an upper midline laparotomy providing good common access to the abdominal cavity in preparation for perforated, ischemic or necrotic bowel.

Conclusion
In conclusion, the combination of a left diaphragmatic hernia, stenoting colon neoplasia and colon perforation make this case unusual, and provide further support to the literature that maybe there is no role for watchful waiting in the case of Morgagni-Larrey hernia.
References
- Testini M, Girardi A, Isernia RM, De Palma A, Catalano G, et al. Emergency surgery due to diaphragmatic hernia: Case series and review. World J Emerg Surg. 2017; 18: 23.
- Mohamed M, Al-Hillan A, Shah J, Zurkovsky E, Asif A, et al. Symptomatic congenital Morgagni hernia presenting as a chest pain: A case report. J Med Case Rep. 2020; 14: 13
- Bettini A, Ulloa JG, Harris H. Appendicitis within Morgagni Hernia and simultaneous Paraesophageal Hernia. BMC Surg. 2015; 15: 15.
- Abraham V, Myla Y, Verghese S, Chandran BS. Morgagni-larrey hernia- A review of 20 cases. Indian J Surg. 2012; 74: 391-395.