
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Extensive cerebral venous thrombosis in a patient with previous COVID-19 infection
Li Wei Heng1; Christopher Yuan Kit Chua2; Ka Zhang2; Ei Zune The2; Vijay K Sharma2
1 Department of Emergency, National University Hospital, Singapore.
2 Division of Neurology, National University Hospital and Yong Loo Lin School of Medicine, National University of Singapore,Singapore.
*Corresponding Author : Heng Li Wei
Department of Emergency, 5 Lower Kent Ridge Road, National University Hospital, Singapore.
Email: liwei.heng1@mohh.com.sg
Received : Apr 15, 2021
Accepted : May 12, 2021
Published : May 17, 2021
Archived : www.jcimcr.org
Copyright : © Heng LW (2021).
Abstract
The coronavirus disease 2019 (COVID-19) has been associated with coagulopathy that can lead to thrombotic complications such as stroke. There are increasing reports of association between active COVID-19 infection and Cerebral Venous Thrombosis (CVT). However, the complication of coagulopathy, like CVT, has only been reported only in active ongoing infections. We report a 30-year-old healthy man who presented with extensive CVT due to previous asymptomatic COVID-19 infection.
Keywords: COVID-19; Computerised tomography; Cerebral venous sinus thrombosis; ‘Thunderclap’ headache; Post infection.
Citation: Heng LW, Chua CYK, Zhang K, The EZ, Sharma VK. Extensive Cerebral Venous Thrombosis in a patient with previous COVID-19 infection. J Clin Images Med Case Rep. 2021; 2(3): 1148.
Introduction
The coronavirus disease 2019 (COVID-19) has been associated with coagulopathy that can lead to thrombotic complications such as stroke. There are increasing reports of association between active COVID-19 infection and Cerebral Venous Thrombosis (CVT). However, the complication of coagulopathy, like CVT, has only been reported only in active ongoing infections. We report a 30-year-old healthy man who presented with extensive CVT due to previous asymptomatic COVID-19 infection.
Case report
A 30-year-old Malay man presented to the emergency department with severe right temporo-parietal headache of sudden-onset for two days. He described the headache as a ‘Thunderclap’, quickly becoming the ‘Worst Headache’ of his life. The headache was associated with nausea, vomiting, lethargy and giddiness. However, there was no photophobia, phonophobia, weakness of extremities or disturbances in vision or speech. The severity of headache was relieved slightly with paracetamol. He denied any recent fall or head injury. He had not suffered from fever or any respiratory illness during past 6 months. He did not suffer from any chronic illness. However, he had been smoking about 10 sticks per day for past four years.
On arrival, he was fully conscious and oriented. He was afebrile and had a regular pulse at 78 beats per minute and a blood pressure of 136/85 mmHg. Neurological examination was unremarkable. His fundus examination did not reveal any papilloedema and there were no signs of meningeal irritation. The rest of his systemic examination was normal.
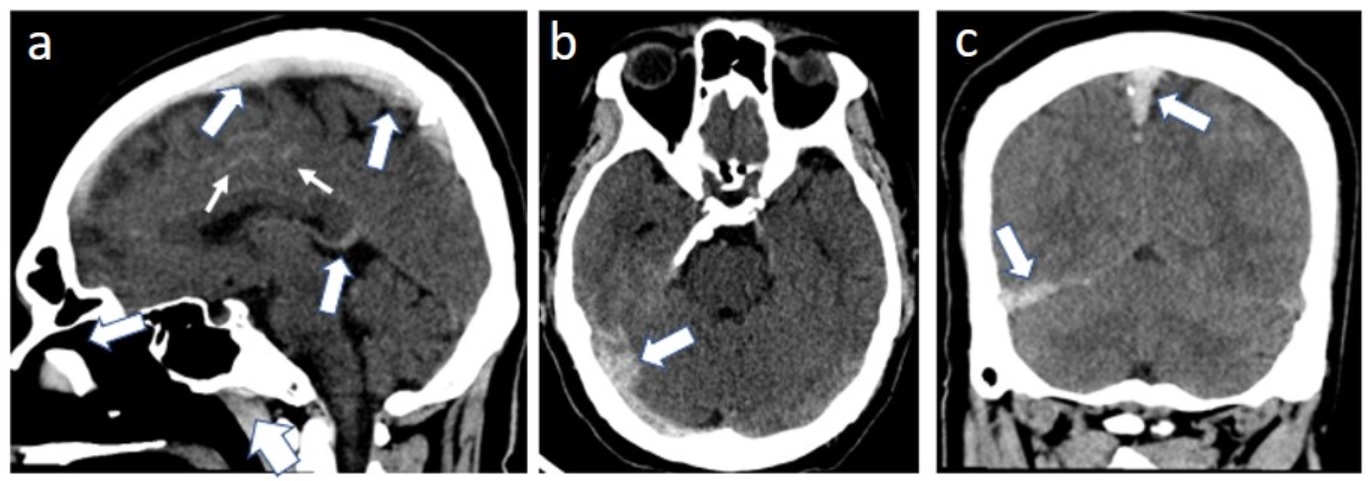
An urgent computed tomography (CT) of the brain was done and it showed scattered sulcal subarachnoid haemorrhages along both cerebral convexities (Figure 1a) without any parenchymal abnormalities. Subsequent CT angiography did not reveal any aneurysm, but instead revealed extensive Cerebral Venous Thrombosis (CVT) involving the superior sagittal (Figure 1a), right transverse (Figure 1b), right sigmoid sinuses, right internal jugular vein (Figure 1c), torcula (Figure 1c) and bilateral cortical veins.
After sending his blood samples for thrombophilic disorders, intravenous heparin infusion was started with a therapeutic target of maintaining activated partial thromboplastin time 1.5 to 2 times of the control value. His admission total white cell count was elevated at 19.36 x 109/L (neutrophilic), but haemoglobin, platelet count and coagulation profile (PT, INR, APTT) were normal. Anti-cardiolipin IgM was at an indeterminate level of 12.76 MPL (negative <12.5 MPL, positive >20 MPL) but IgG was negative at 14.63 GPL (negative <15 GPL, positive >20 GPL). Lupus anticoagulant and B2-glycoprotein IgM and IgG were negative. ESR was within normal limits and anti-nuclear antibody was <1:80. The blood levels for protein C, protein S, antithrombin-III, D-dimer and lactate dehydrogenase were within normal limits. Factor V Leiden gene test was normal and viral hepatitis B and C screens were negative. Interestingly, the serology for COVID-19 antibodies was positive but two nasopharyngeal swabs for COVID-19 infection, done 24 hours apart, as well as his chest X-ray were negative for an active infection. The COVID-19 serology was done in view of the recent outbreak in Singapore.
His further stay in the hospital was unremarkable. His symptoms improved rapidly with intravenous heparin infusion, and it was converted to oral warfarin on day 6. He was subsequently discharged home.
Discussion
We describe the clinical, imaging and laboratory findings of extensive CVT in an otherwise healthy young man. Contrary to the previous reports of CVT with concurrent COVID-19 infection, our patient’s blood tested positive for COVID-19 antibodies despite no history of any such infection during past 6 months.
Association between acute COVID-19 infection and coagulopathy has been reported. Accordingly, elevated levels of D-dimer, fibrinogen and fibrin/fibrinogen degradation products, disseminated intravascular coagulation, thrombocytopenia, and presence of antiphospholipid antibodies were found to correlate with the severity of COVID-19 [1,2] as well as various complications including venous thromboembolism, myocardial infarction and stroke [3,4]. Furthermore, some case reports and series describing CVT associated with COVID-19 have been published recently [5-9]. A recent study compared the demographics, clinical and radiological characteristics, risk factors and outcome between patients with CVT with concurrent COVID-19 infection with those who developed CVT prior to the arrival of COVID-19 [10].
A recent systematic review by Tu et al reported that majority COVID-19 cases who developed CVT were relatively young and healthy individuals with minimal comorbidities. The study suggested that hypercoagulable state may develop even among patient with mild infection. The median days to CVT diagnosis was 7 days from the onset of COVID-19 symptoms [11]. Our patient did not experience any symptoms related to COVID-19 in recent past and 2 nasopharyngeal swabs were negative. COVID-19 antibodies were tested only because of the absence of any thrombophilic state and absence of any co-morbidity.
The mechanisms through which COVID-19 triggers CVT remain debatable. In addition to sepsis and various known thrombophilic states, cytokine release, systemic inflammation, endothelial injury, prothrombotic effects of unopposed angiotensin II and direct neuro-invasion of the virus are believed to cause a hypercoagulable state during acute COVID-19 infection. [12-14] Except for the indeterminate levels of anti-cardiolipin IgM, we could not find any other contributing factor for CVT in our patient. Our patient did have an elevated total white cell count, but it promptly improved by the next check and he did not have any fever nor evidence of infection. Although, the mechanism remains obscure, we hypothesize that an asymptomatic recent COVID-19 infection played a major causative role in the development of extensive CVT in our patient.
Early initiation of anticoagulation therapy led to rapid recovery in our patient. Our case highlights that venous thrombotic events may occur even among patients who have recovered from COVID-19, not just in patients with ongoing infection.
Declaration: There are no affiliations or financial involvement with any commercial organisation with a direct financial interest in the subject or materials discussed in the manuscript.
What is known: The complication of coagulopathy, like CVT, has only been reported only in active ongoing COVID-19 infections.
What is new: We report a case of CVT occurring in a healthy young male patient who had a previous asymptomatic COVID-19 infection. COVID-19 serology was positive, but two COVID-19 PCR swabs done 24hrs apart whilst inpatient were negative.
Key message: The healthcare industry would be seeing an increasing number of patients who recovered from COVID. Therefore, we believe that our article would be of interest to clinicians in the management of patients who had previous COVID-19 infection, presenting with headache, even if they are young and healthy.
References
- Han H, Yang L, Liu R, Fang L, Kai-Lang W, et al. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin Chem Lab Med. 2020; 58: 1116-1120.
- Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020; 18: 844-847.
- Helms J, Tacquard C, Severac F, Ian LL, Mickaël O, et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020; 46: 1089-1098.
- Oxley TJ, Mocco J, Majidi S, Christopher PK, Hazem S, et al. Large-Vessel Stroke as a Presenting Feature of Covid-19 in the Young. N Engl J Med. 2020; 382: e60.
- Cavalcanti DD, Raz E, Shapiro M, Dehkharghani S, Yaghi S, et al. Cerebral Venous Thrombosis Associated with COVID-19. AJNR Am J Neuroradiol. 2020; 41: 1370-1376.
- Poillon G, Obadia M, Perrin M, Savatovsky J, Lecler A. Cerebral venous thrombosis associated with COVID-19 infection: Causality or coincidence?. J Neuroradiol. 2020: S0150-9861(20)30167-X.
- Shakibajahromi B, Borhani-Haghighi A, Haseli S, Mowla A. Cerebral venous sinus thrombosis might be under-diagnosed in the COVID-19 era. E Neurological Sci. 2020: 100256.
- Chougar L, Mathon B, Weiss N, Degos V, Shor N. Atypical Deep Cerebral Vein Thrombosis with Hemorrhagic Venous Infarction in a Patient Positive for COVID-19. AJNR Am J Neuroradiol. 2020; 41: 1377-1379.
- Hemasian H, Ansari B. First case of Covid-19 presented with cerebral venous thrombosis: A rare and dreaded case. Rev Neurol (Paris). 2020; 176: 521-523.
- Mowla A, Shakibajahromi B, Shahjouei S, Afshin BH, Nasrin R, et al. Cerebral venous sinus thrombosis associated with SARS-CoV-2; A multinational case series. J Neurol Sci. 2020; 419: 117183.
- Tu TM, Goh C, Tan YK, Leow AS, Pang YZ, Chien J, et al. Cerebral venous thrombosis in patients with COVID-19 infection: A case series and systematic review. J Stroke Cerebrovasc Dis. 2020; 29: 105379.
- Liu PP, Blet A, Smyth D, Li H. The Science Underlying COVID-19: Implications for the Cardiovascular System. Circulation. 2020; 142: 68-78.
- Ortel TL. Acquired thrombotic risk factors in the critical care setting. Crit Care Med. 2010; 38: S43-50.
- Paniz-Mondolfi A, Bryce C, Grimes Z, Ronald EG, Jason R, et al. Central nervous system involvement by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). J Med Virol. 2020; 92: 699-702.