
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Severe asthma that was endotracheally intubated 16 times in 20 years
Luis J Nannini
Pulmonology Hospital “E Perón” of Granadero Baigorria. Argentina. Faculty of Medical Sciences, National University of Rosario, Argentina.
*Corresponding Author : Luis J Nannini
Pulmonology Hospital “E Perón” of Granadero Baigorria. Argentina. Faculty of Medical Sciences, National University of Rosario, Argentina.
Email: ljnannini@hotmail.com
Received : Apr 15, 2021
Accepted : May 12, 2021
Published : May 17, 2021
Archived : www.jcimcr.org
Copyright : © Nannini LJ (2021).
Abstract
Introduction: Severe asthma is a complex airway disease characterised by multiple aggravating-factors, and frequent comorbidities. Poor asthma control does not always correspond to the severity of airflow obstruction. One cause of disproportionate breathlessness in asthma is dysfunctional breathing/hyperventilation syndrome which is increasingly recognized.
Case study: This female individual arrived at our asthma centre for the first time, coming from a primary care site 20 years ago. During the past 20 years she was intubated 16 times. Airway obstruction was never assessed surrounding the acute asthma episodes. Asthma diagnosis was confirmed by spirometry many times during routine visits at the asthma centre, where she never came to our asthma centre during an acute asthma exacerbation. Despite warranting the availability of controller medication with high ICS dose plus LABA, she repeated the episodes of severe dyspnoea requiring endotracheal intubations.
Results: At a routine outpatient visit to our asthma centre for claiming her asthma medication, she developed an extreme dyspnoea as it occurred so many times earlier, using accessory respiratory muscles. The modified Borg scale for dyspnoea was 9/10. Pulse oximetry showed 96% O2 saturation breathing at room air. Baseline FEV1 was 1.96 L. Dyspnoea did not improve after 30 minutes of treatment. However, the FEV1 increased 29% to 2.53 L (96% predicted). Relaxation respiratory techniques began and the extreme dyspnoea slowly disappeared.
Conclusion: Hyperventilation syndrome was confirmed with a score 32 with the Nijmegen Questionnaire (normal <23). Hyperventilation syndrome could coexist with severe asthma in 47% of cases.
Keywords: Asthma; Asthma primary care; Hyperventilation syndrome.
Citation: Nannini LJ. Severe asthma that was endotracheally intubated 16 times in 20 years. J Clin Images Med Case Rep. 2021; 2(3): 1150.
Introduction
Severe asthma is a complex and heterogeneous airway disease characterised by multiple aggravating-factors, several clinical phenotypes and biological endotypes, and frequent comorbidities [1]. Poor asthma control is manifested by residual symptom burden following treatment, but does not always correspond to the severity of airflow obstruction. One cause of disproportionate breathlessness in asthma is dysfunctional breathing, which is increasingly recognized but remains poorly understood [2].
Case study
The individual saw the figure and signed the informed consent for publication. She is a non-smoker female 40 years old. She has a history of asthma since the first year of life. She arrived at our asthma centre for the first time, coming from a primary care setting 20 years ago. She had frequent acute severe asthma exacerbations requiring endotracheal intubations because of extreme dyspnoea. During the past 20 years she was intubated 16 times. Airway obstruction was never assessed surrounding the acute asthma episodes; firstly, due to the sudden onset of life-threatening catastrophic attack, and secondly because all the episodes occurred in primary health care resources that do not measure airway obstruction. Asthma diagnosis was confirmed by spirometry many times during routine visits at the asthma centre, where she never came during an acute asthma exacerbation. Despite warranting the availability of controller medication with high ICS dose plus LABA, she repeated the episodes of severe dyspnoea requiring endotracheal intubations. We indicated omalizumab every 4 weeks. A reduction in corticosteroid use was achieved; but she anyway needed two more endotracheal intubations in another primary health care setting without objectively assessing the severity of the attack. I had given her a sort of red alert card to ensure a rapid assistance upon arrival to Emergency Services 20 years ago.
Results
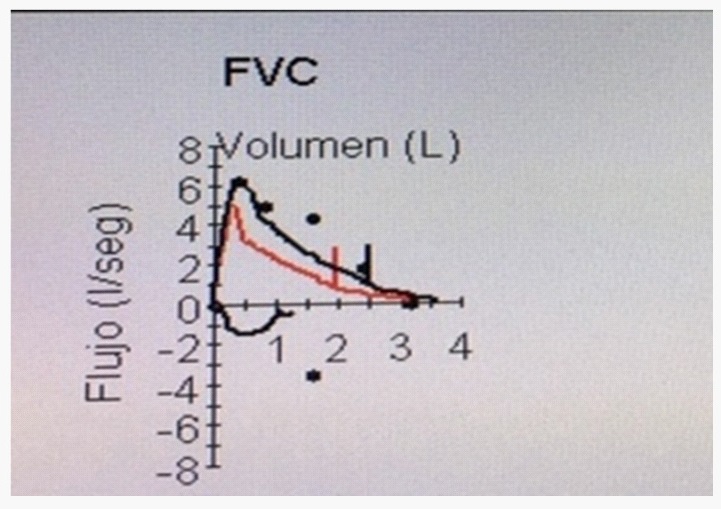
The red alert card was discarded because we disclosed what happened during her asthma exacerbations as follows: 1) One of the last episodes the individual was sent with endotracheal intubation to our ICU and while she was under mechanical ventilation, the airway pressures were amazingly normal, without Auto-Peep. She could be extubated within the first 24 hours. Before discharge, the lung function test showed a mild obstruction with a great response to bronchodilator. Two months later, a bronchial hyperresponsiveness test with histamine was performed and a Pc20= 0.16 mg/ml was registered at our asthma centre. 2) At a routine outpatient visit to our asthma centre for claiming her asthma medication, she developed an extreme dyspnoea as it occurred so many times earlier, using accessory respiratory muscles, plus nasal flaring, and upper thoracic breathing. Heart rate 98 bpm, respiratory rate 28/min, 130/82 mm Hg arterial pressure with pulsus paradoxus less than 10 mm Hg; and at auscultation: mild bilateral wheezing. She could speak slowly. The modified Borg scale for dyspnoea was 9/10. Pulse oximetry showed 96% O2 saturation breathing at room air. Arterial blood gas analysis showed a mild hypocapnia. We performed a baseline spirometry before beginning acute asthma treatment. Incredibly, the baseline FEV1 was 1.96 L (74% predicted). The flow-volume curve did not show upper airway obstruction. After 30 minutes of treatment with inhaled budesonide/formoterol, intravenous dexamethasone 8 mg, and salbutamol; the dyspnoea did not improve. However, the FEV1increased 29% to 2.53 L (96% predicted) as it was shown in Figure 1. A thoracic CT scan was performed to rule out the diagnosis of pulmonary embolism, pneumothorax or other cause of dyspnoea. The CT was normal with a mild hyperinflation. Relaxation respiratory techniques began and the extreme dyspnoea slowly disappeared. 3) Hyperventilation syndrome was confirmed with a score 32 with the Nijmegen Questionnaire [3]. The normal score should be less than 23. We measured our dyspnoea index perception [4], and she had a higher index in comparison with all the other individuals who had history of near fatal asthma attack.
During 2019 oral corticosteroids was tapered to cero. She did not have severe exacerbations, neither hyperventilation episodes since October 2019 anymore. She received combined budesonide/formoterol four doses per day and as needed; and performs daily respiratory relaxation sessions [5]. The Nijmegen Questionnaire was 30 at February 2021; but with asthma totally controlled and normal lung function.
Conclusion
Airway obstruction assessment during acute asthma circumstances should be performed because many comorbidities of severe asthma can mimic severe life-threatening asthma. Hyperventilation syndrome could coexist with severe asthma in 47% of cases [6].The Nijmegen Questionnaire has a specificity of 95% [7]. Dysfunctional breathing and hyperventilation syndrome were mentioned in the International Recommendations for Severe asthma, such as GINA [8], ATS/ERS [9]; but Nijmegen Questionnaire is not included as a diagnostic tool.
References
- Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, et al. International ERS/ATS guidelines on definition, evaluation and treatment ofsevere asthma. Eur. Respir. J 2014; 43: 343–373.
- Porsbjerg C, Menzies-Gow A. Co-morbidities in severe asthma: Clinical impact and management. Respirology. 2017; 22: 651-661.
- van Dixhoorn J, Folgering H. The Nijmegen Questionnaire and dysfunctional breathing. ERJ Open Res. 2015; 1: 00001-2015.
- Nannini LJ, Zaietta GA, Guerrera AJ, Varela JA, Fernández OM. Breath-holding test in subjects with near-fatal asthma. A new index for dyspnea perception. Respir Med. 2007; 101: 246-253.
- Holloway EA, West RJ. Integrated breathing and relaxation training (the Papworth method) for adults with asthma in primary care: A randomised controlled trial. Thorax. 2007; 62: 1039-1042.
- Denton E, Bondarenko J, Tay T, Lee J, Radhakrishna N, et al. Factors Associated with Dysfunctional Breathing in Patients with Difficult to Treat Asthma. J Allergy Clin Immunol Pract. 2019; 7: 1471-1476.
- van Dixhoorn J, Duivenvoorden HJ. Efficacy of Nijmegen Questionnaire in recognition of the hyperventilation syndrome. J Psychosom Res. 1985; 29: 199-206.
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2020.
- Holguin F, Cardet JC, Chung KF, et al. Management of severe asthma: A EuropeanRespiratory Society/American Thoracic Society guideline. Eur Respir J. 2020; 55: 1900588.