
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Mediastinal eggshell calcifications
Lisa N Glass1*; Joseph Delio1; Jalil E Ahari2
1Pulmonary Disease and Critical Care Medicine, The George Washington University School of Medicine and Health Sciences, USA.
2Associate Professor in the Division of Pulmonary, Critical Care and Sleep Disorders Medicine, The George Washington University School of Medicine and Health Sciences, USA.
*Corresponding Author : Lisa N Glass
Pulmonary Disease and Critical Care Medicine, The George Washington University School of Medicine and Health Sciences, USA.
Email: lisaglass@gwu.edu
Received : Apr 16, 2021
Accepted : May 17, 2021
Published : May 20, 2021
Archived : www.jcimcr.org
Copyright : © Glass LN (2021).
Citation: Glass LN, Delio J, Ahari JE. Mediastinal eggshell calcifications. J Clin Images Med Case Rep. 2021; 2(3): 1153.
Presentation
A 71-year-old man, who is non-smoker with past medical history notable for hypertension and right lower extremity deep vein thrombosis three years prior, presented with progressive dyspnea on exertion of two weeks duration. He did not have any chest pain; heart rate and blood pressure were normal. His DVT had occurred in the setting of trauma, where he was injured by a falling tree. He was treated with anticoagulation for six months and recovered.
Assessement
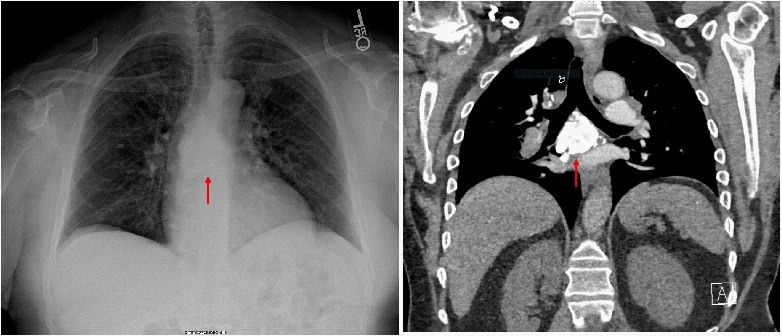
Chest X-ray showed mediastinal calcification (Figure A, red arrow). D-dimer was performed, which was elevated to 8.34 mcg/mL. CT angiogram demonstrated pulmonary emboli in the right and left pulmonary arteries. Troponin was not detectable and Brain Natriurietic Peptide (BNP) was mildly elevated at 323 pg/mL. The assessment of the Right Ventricle (RV) was limited on transthoracic echocardiogram, but did not indicate abnormal RV systolic function. CT angiogram also showed enlarged, calcified subcarinal lymph nodes and sub-centimeter calcified nodules (Figure B, Red Arrow). A CT scan 1-year prior showed similar findings, consistent with sequela of granulomatous disdisease. He was started on apixaban for anticoagulation. He was noted to have improvement in his dyspnea with anticoagulation.
Diagnosis
The differential diagnosis for eggshell calcification on Chest X-ray is broad. Infectious process associated with eggshell calcification include fungal infections histoplasmosis, blastomycosis and tuberculosis [1]. Associated occupational exposures include silicosis and coal workers’ pneumoconiosis [2,3]. Associated diffuse parenchymal lung diseases include sarcoidosis, amyloidosis and systemic sclerosis [4].
Management
Eggshell calcifications may be associated with various disease processes. In this case, a history of granulomatous disease was suspected. Dyspnea improved with therapeutic anticoagulation for pulmonary embolism. As per Fleischner society guidelines, further imaging and workup was not indicated [5].
References
- Gross BH, Schneider HJ, Proto AV. Eggshell calcification of lymph nodes: An update. AJR Am J Roentgenol. 1980; 135: 1265-1268.
- Baldwin DR, Lambert L, Pantin CF, Prowse K, Cole RB. Silicosis presenting as bilateral hilar lymphadenopathy. Thorax. 1996; 51: 1165-1167.
- Bhawna S, Ojha UC, Kumar S, Gupta R, Gothi D, Pal RS. Spectrum of high resolution computed tomography findings in occupational lung disease: Experience in a tertiary care institute. J Clin Imaging Sci. 2013, 3: 64-7514.
- Silva M, Nunes H, Valeyre D, Sverzellati N. Imaging of Sarcoidosis. Clin Rev Allergy Immunol. 2015; 49: 45-53.
- MacMahon H, Naidich DP, Goo JM, Lee KS, Leung ANC, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society. Radiology. 2017; 284: 228-243.