
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
High-Tech radiotherapy for primary prostate cancers and synchronous other tumor in elderly
Alessia Surgo 1 ; Ilaria Bonaparte 1 ; Fabiana Gregucci 1 *; Roberta Carbonara 1 ; Maria Paola Ciliberti 1 ; Morena Caliandro 1 ; Elena Ludovico 2 ; Roberto Calbi 2 ; Alessandro Verbo 3 ; Vincenzo D’Angelo 4 ; Marcello Scarcia 5 ; Giuseppe Mario Ludovico 5 ; Romeo Armeno 6 ; Letizia Laera 7 ; Giammarco Surico 7 ; Alba Fiorentino 1
1 Radiation Oncology Department, General Regional Hospital F. Miulli, Acquaviva delle Fonti-Bari (BA) Italy.
2 Radiology Department, General Regional Hospital F. Miulli, Acquaviva delle Fonti-Bari (BA) Italy.
3 Surgery Department, General Regional Hospital F. Miulli, Acquaviva delle Fonti-Bari (BA) Italy.
4 Neurosurgery Department, General Regional Hospital F. Miulli, Acquaviva delle Fonti-Bari (BA) Italy.
5 Urology Department, General Regional Hospital F. Miulli, Acquaviva delle Fonti-Bari (BA) Italy
6 ASM Matera, Ospedale Madonna delle Grazie, Italy
7 Medical Oncology Department, General Regional Hospital F. Miulli, Acquaviva delle Fonti-Bari (BA) Italy
*Corresponding Author: Fabiana Gregucci
Radiation Oncology Department, General Regional
Hospital F. Miulli, Strada Provinciale 127, 70020,
Acquaviva delle Fonti-Bari (BA) Italy.
Email: fabianagregucci@gmail.com
Received : Apr 19, 2021
Accepted : May 19, 2021
Published : May 21, 2021
Archived : www.jcimcr.org
Copyright : © Gregucci F (2021).
Abstract
Aims: To report feasibility and efficacy of high-tech Radiotherapy (RT) for the treatment of synchronous Multiple Primary Malignancies (sMPM) for elderly patients with primary Prostate Cancer (PC).
Methods: Two elderly patients with PC and synchronous Anal Cancer (AC) and sacrum chordoma, respectively, were described.
The first one was treated with radical radio-chemotherapy. A total dose of 70 Gy / 65.5 Gy (28 fractions) was prescribed to prostate/ seminal vesicles, and concomitantly, 56 Gy / 50.4 Gy / 45 Gy were prescribed to tumor, anal canal/mesorectum/pelvic nodes, and inguinal nodes, respectively.
For the second case, after resection of chordoma, adjuvant and prostate radical RT (65.5 Gy / 70 Gy) in 28 fractions were used.
In both cases, Volumetric-Arc RT was performed.
Results: Patients completed the planned treatment without severe toxicities. After a median follow-up of 12 months, no sign of PC and a controlled/reduction of chordoma/AC were observed.
Conclusion: High-tech RT is safe and effective for sMPM elderly patients.
Keywords: Synchronous cancers; Elderly; Treatment; Radiotherapy; Multidisciplinary evaluation.
Citation: Surgo A, Bonaparte I, Gregucci F, Carbonara R, Ciliberti MP. High-Tech radiotherapy for primary prostate cancers and synchronous other tumor in elderly. J Clin Images Med Case Rep. 2021; 2(3): 1157.
Introduction
Synchronous Multiple Primary Malignancies (sMPM), defined as two-more primary tumors occurring in the same patient, are rare clinical presentations. A temporal classification describes sMPM as synchronous or metachronous, depending on time of diagnosis of the second tumor inferior or superior at 6 months from the first.
Despite the limited data, for some categories few details are available, for example among the synchronous colorectal neoplasms in which the incidence is estimated between 0.17%- 0.69%, [1,2]. Recently, Corvino et al reported a prevalence of sMPM of 3.6% and the most frequent first primary tumors were melanoma (17.8%), lymphoma (15.6%), and prostate carcinoma (15.6%). Moreover, among sMPM patients, the relative risk of other tumors increased with patient age and male sex [3].
Surgery, radiotherapy (RT) with/without chemo/hormonaltherapy are classically considered in the armamentarium of the cancer battle. While the existing guidelines report the specific recommendations for the treatment of each single primary tumor, there are no recommendations regarding the management of the synchronous cancers, especially for older patients. In fact, the cancer development and the normal tissue radiosensitivity or response could be affected by the aging process in this setting of patients. Due to the physiological organ alterations and the decreasing of functional reserve, the elderly could tolerate a lower dose of RT, with the consequently increasing of side effects. Thus, regarding RT, high technological improvements, by means of Intensity Modulated RT (IMRT) or Volumetric Modulated Arc RT (VMAT), are available in the clinical practice. Their delivering modality reduce the risk of side effects decreasing the normal tissues irradiation and guaranteeing a better tumor dose distribution. As shown in literature, high-tech RT is advantageous for elderly [9].
Based on these data, it is easy to predict that with the improving in tumor staging (Computed Tomography CT and or CTPET), the increasing in life expectancy, the increasing of cancer population and the most frequent prostate cancer as primary tumor in patients over 65 years old, in the next future the incidence of sMPM will grow up, especially in the elderly population.
Thus, due to the lack of either specific guidelines or individuals’ clinical experiences relative to these clinical presentations, here we reported the feasibility, efficacy, and tolerability of high-tech RT for the treatment of synchronous tumors in two elderly patients with primary prostate cancer.
Case 1
Presenting concerns, clinical findings and diagnostic assessment
The story of 71-years-old patient (hypertension and KPS 90) started in December 2019 with an increase of PSA (9 ng/ml). During the urological evaluation, an ulcerated mass at the anal canal wall and mild prostatemegaly with a palpable suspicious nodule in the left prostate lobe, without any signs of the extracapsular extension were observed. A pelvic Magnetic Resonance Imaging (MRI), rectal colonoscopy and biopsy of prostate were proposed.
Subsequent colonoscopy confirmed the presence of a suspicious lesion on the anal canal, and the histological examination confirmed the Squamous Cell Anal Carcinoma (SCAC).
In April 2020, an MRI confirmed an infiltrative lesion of the anal canal with a maximum diameter of 33 cm, with a highgrade suspicion of sphincter infiltration and no clear lymphadenopathies in the mesorectum and or in the pelvis. A Total-Body (TB) CT was performed and it excluded distant metastases.
Patient refused the prostatic biopsy and for this reason a PET-Choline was scheduled and it showed pathological lesion on the right lobe of prostate gland (SUV 7.2) without nodal involvement.
Therefore, our patient had a synchronous cT2N0M0 prostate adenocarcinoma and stage IIIa cT2N1M0 SCAC.
Therapeutic intervention: Multidisciplinary approach
A multidisciplinary team which included surgical, medical, and radiation oncologists evaluated this case and agreed a decision to propose to the patient a radical concurrent radio-chemotherapy for SCAC and definitive RT for prostate cancer.
Treatment
From April to June 2020 the patient received radio-chemotherapy.
A 2 mm slice thickness CT simulation scan in prone position, with Bellyboard™ (Civco) device was acquired. In order to obtain reproducible volumes of bladder for each fraction, patient was educated at the use of drinking 500 ml of water 30 minutes before the scan for bladder filling.
Concerning delineation, Clinical Target Volume (CTV)-1 consisted of the prostate gland, CTV-2 seminal vesicles, CTV-3 canal anal tumor, CTV-4, included the anal canal with the perineum, the entire mesorectum (perirectal nodal region) to the pelvic floor, the pelvic nodal regions (internal ili-ac, external iliac, and presacral), CTV-5 included inguinal nodes. For a definition of the target vol-umes, the anorectal contouring atlas published by RTOG was used.
Planning Target Volumes (PTV1-5) was generated adding to CTV a 0.5 cm margin in all direction.
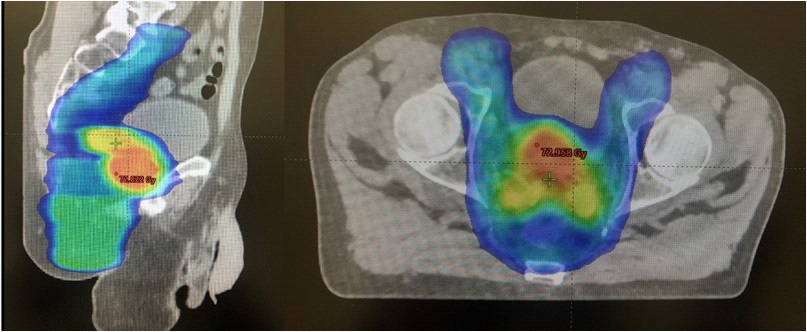
A total dose of 70 Gy and 65.5 Gy (28 fractions) were prescribed to PTV1 and 2, respectively. For anal tumor, a total dose of 56 Gy, 50.4 Gy and 45 Gy in 28 fractions were prescribed to PTV3, PTV4, PTV5, respectively. A Simultaneous Integrated Boost (SIB)-VMAT plan was delivered with 4 complete coplanar arcs, optimized simultaneously and delivered with opposite rotation. The plan was created using 6-MV photon beams commissioned for a Varian TrueBeam Linac (Varian Medi-cal System, Palo Alto, California, USA) (Figure 1). Daily Image Guided RT (IGRT) with Cone Beam CT (CBCT) and Surface Guided RT (SGRT) with Align RT, were used to set-up control and beam-on.
Concurrent chemotherapy with Cisplatin (60 mg/m2 every 21 days) plus Capecitabine (825 mg/m2 twice daily for 5 days/ week) was performed.
Treatment response and outcome
Patient completed the planned treatment without any interruption, with G2 Gastro-Intestinal (GI) and genito-urinary (GU) and G3 dermatitis acute toxicity and G1 anemia (Hb 10.2 g/dl).
At the time of this analysis, PSA was 1.47 ng/ml (December 2020, 7 months after RT), MRI showed SCAC major response but persistence of tumor. Further investigations with TB-CT, FDG-PET, anoscopy and biopsy revealed no evidence of tumor. No RT late side effects were registered.
Case 2
Presenting concerns, clinical findings and diagnostic assessment
In March 2019, for an increase of PSA (7 ng/ml), a 76-yearsold patient without comorbidities, underwent to urologic evaluation and consequent prostatic biopsy. The diagnosis was adenocarcinoma of prostate gland with Gleason Score of 3+3 (Group-1). In April 2019 the patient underwent to pelvic MRI to a better definition of the low-risk prostate cancer. MRI confirmed the prostate cancer without capsular infiltration and pelvic node positive, but it showed a 6 cm mass that occupied the sacrum (S2-S4) and the pelvis, similar to a sacral chordoma. A TB-CT excluded other pathological lesions.
Therapeutic intervention: Multidisciplinary approach
His case was discussed at the multidisciplinary tumor board and the decision was: surgical approach by neuro- and colorectal-surgeons followed by adjuvant RT for the chordoma and concomitantly radical RT for prostate cancer.
Carbon ion was proposed to patient who refused for organizational issue.
Treatments
In May 2019, patient underwent to surgical intervention by neurosurgeon for sacral mass and colorectal surgeon for the pelvic mass, without side effect except sacral pain. Histological examination reveals a chordoma of the sacral bone.
Post-operative pelvic MRI showed the partial removal on the infiltrating bone, but the complete removal of the pelvic and sacral mass.
After 2 months from surgery, from July to September 2019 the patient received RT.
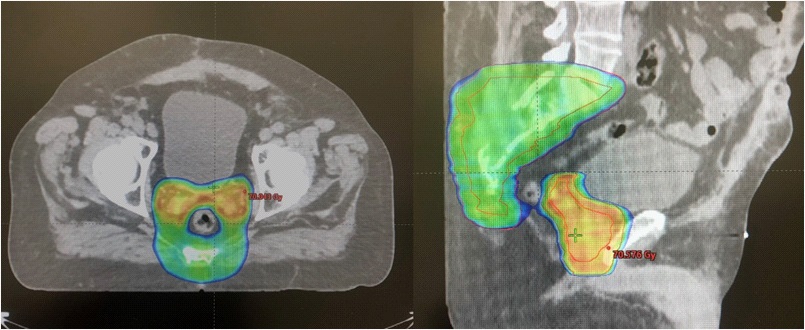
A 2 mm slice thickness CT simulation scan in supine position, with Combifix (Civco) device was acquired. In order to obtain reproducible volumes of bladder and rectum for each fraction, patient was educated at the use of fleet enemas 2 hours before the CT scan for rectal emptying, and he was required to drink 500 ml of water 30 minutes before the scan for bladder filling. Concerning target volume delineation, CTV-1 consisted of the prostate gland and CTV2 consisted of sacral tumor site. PTV1-2 was generated adding to CTV-1 a 0.5 cm margin in all direction except posteriorly, where a 0.3 cm margin, while adding a CTV-2 a 1 cm was used. A total dose of 70 Gy and 65.5 Gy (28 fractions) were prescribed to PTV1 and 2, respectively. SIB-VMAT was delivered with 3 coplanar arcs, optimized simultaneously and delivered with opposite rotation. The plan was created using 6-MV photon beams commissioned for a Varian TrueBeam Linac (Varian Medical System, Palo Alto, California, USA) (Figure 2). Daily IGRT with CBCT and SGRT with Align RT, were used to set-up control and beam-on.
Treatment response and outcome
Patient completed the planned treatment without any interruption, with G1 GI and GU acute toxicity and no evidence of any G3 or higher acute adverse event. The first post-RT (November 2019) PSA was 0.6 ng/ml. At the moment of this analysis, PSA was 0.2 ng/ml (December 2020, 1 years after RT) and MRI showed stable disease for residual chordoma. No RT late side effects were registered. Patient suffered from sacral pain after surgery (VAS max 7) controlled by medical therapy.
Discussion
Advancing age is a high-risk factor for cancer, with people over 65 years accounting for 60% of newly diagnosed malignancies [6]. The incidence of cancer and its mortality in elderly are 10 and 16 times greater than in younger, respectively [6].
Prostate cancer, the 2nd most common tumor in patients over 65, is the most frequent primary tumor in sMPM patients [3]. Moreover, despite sMPM are rare entity, in the next decades, due to several considerations, their incidence will grow up.
To date, no guidelines are recommended for elderly people with synchronous tumors. In general, RT is one of the cancer weapons, reporting a benefit in terms of overall survival and disease free survival [7].
The advances in RT, including IMRT or VMAT, represent an option that provides high precision delivery, avoiding organ at risks [4,5].
This RT treatment approach was here reported in 2 elderly patients affected by prostate cancer and SCAC and chordoma of the sacrum, respectively.
The present cases reported the feasibility and efficacy of radical high-tech RT in prostate/anal cancer and prostate/chordoma, without severe acute and late toxicities.
The most of papers published about the management of sMPM regard rectal and prostate cancer. The published literature suggests that the approach to synchronous rectal and prostate cancer has moved away from a surgery only approach [8-10]. Prostate surgery after neoadjuvant RT increases the technical difficulty of the prostatectomy and most urologists would avoid it in a previous irradiated field unless no other treatment options are available [10]. For the latter reason, in the present cases, prostate surgery was excluded for our patients in the multidisciplinary board.
Regarding prostate and SCAC, in literature only another case was published about the use of high-tech RT (radical IMRT), reporting similar results [2]. Slavisa et al. prescribed a dose of 69.3 Gy (2.1 Gy/die) on prostate, 59.4 Gy(1.8 Gy/die) on the involved pelvic lymph nodes and primary tumor of the anal canal; 45 Gy on the uninvolved pelvic lymph nodes and 36 Gy(1.8 Gy/die) on the uninvolved inguinal lymph nodes [2]. The authors showed that the patient has tolerated chemoradiotherapy very well, presenting only an acute toxicity G2 erythema in the perianal region, which did not require the suspension of his treatment, and G1 anemia. Two years after the treatment, the restaging CT and MRI scan showed no evidence of the disease and he reported no GI/GU toxicity. These results are similar to the present data: after 6 months from RT, no prostate disease was documented and a reduction of SCAC was reported on MRI, without radiation late side effects.
Moreover, regarding prostate and chordoma, to our knowledge, no data are reported in literature. In the present case, after 18 months, patient is alive without progression of chordoma and no evidence of disease regarding prostate cancer. No acute and late GI/GU effects related to RT superior or equal to G3 was reported.
Conclusion
The association of elderly age and life expectancy are the bases of the increase of cancer rate in elderly and subsequently the increase of sMPM. The proper treatment in elderly with tumor is an oncological challenge, due to the lack of prospective and randomized data in this setting of patients with a single tumor. For elderly sMPM, data are absent. The reported two cases enhanced the possi-bility to use high-tech RT for the cure of these patients without reducing quality of life, due to side effects.
Declarations
Conflict of interest: The authors declare that they have no conflict of interest.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
- Lasser A. Synchronous primary adenocarcinomas of the colon and rectum. Diseases of the Colon and Rectum. 1978; 21: 20– 22.
- Slavisa T, Wolfgang RA. Definitive IMRT-SIB with Concomitant Chemotherapy for Syn-chronous Locally Advanced Anal Canal Cancer and Prostate Cancer. Case Reports in Oncological Medicine. 2018; 6101759.
- Corvino C, Setola AV, Sandomenico F, et al. Synchronous tumours detected during cancer patient staging: Prevalence and patterns of occurrence in multidetector computed tomography. Pol J Radiol. 2020; 85: 261-e270.
- Fiorentino A, Gregucci F, Mazzola R, et al. Intensity-modulated radiotherapy and hypofractionated volumetric modulated arc therapy for elderly patients with breast cancer: Compari-son of acute and late toxicities. Radiol Med. 2019; 124: 309-314.
- Gregucci F, Fiorentino A, Corradini S, et al. Linac-based radiosurgery or fractionated stereo-tactic radiotherapy with flattening filter-free volumetric modulated arc therapy in elderly patients: A mono-institutional experience on 110 brain metastases. Strahlenther Onkol. 2019; 195: 218-225.
- Berger NA, Savvides P, Koroukian SM, et al. Cancer in the elderly. Trans Am Clin Climatol Assoc. 2006; 117: 147-155.
- Hanna TP, Shafiq J, Delaney GP, et al. The population benefit of evidence-based radiother-apy: 5-Year local control and overall survival benefits. Radiother Oncol. 2018; 126: 191-197.
- Lin C, Hua H, Lin J, et al (2011) Synchronous primary carcinomas of the rectum and pros-tate: Report of three cases. Oncol Lett. 2011; 2: 817–819.
- Lavan NA, Kavanagh DO, Martin J, et al. The curative management of synchronous rectal and prostate cancer. Br J Radiol. 2016; 89: 20150292.
- Tey YQ, Ravi K, Chonget CS et al. Management of locally advanced synchronous colorec-tal and prostate cancers. Medicine. 2020; 99: 22.