
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
A continuous cough after COVID-19
Lisa N Glass 1 *; Sandrine Hanna 1 ; John P Lichtenberger 2 ; Ivana Milojevic 3 ; Jalil E Ahari 4
1 Pulmonary Disease and Critical Care Medicine, The George Washington University School of Medicine and Health Sciences, USA.
2 Chief of Thoracic Imaging, The George Washington University Medical Faculty Associates, USA.
3 Assistant Professor, Division of Pulmonary, Critical Care and Sleep Disorders Medicine, The George Washington University School of Medicine and Health Sciences, USA.
4 Associate Professor in the Division of Pulmonary, Critical Care and Sleep Disorders Medicine, The George Washington University School of Medicine and Health Sciences, USA.
*Corresponding Author: Lisa N Glass
Pulmonary Disease and Critical Care Medicine, The
George Washington University School of Medicine
and Health Sciences, USA.
Email: lisaglass@gwu.edu
Received : Apr 17, 2021
Accepted : May 19, 2021
Published : May 21, 2021
Archived : www.jcimcr.org
Copyright : © Glass LN (2021).
Abstract
Organizing pneumonia is a process of lung parenchymal injury caused by multiple etiologies. Although organizing pneumonia may be an idiopathic process, it usually occurs secondary to infection, aspiration, autoimmune disease, and after organ transplantation or radiation. We present a case of organizing pneumona after confirmed SARS-CoV-2 (COVID-19) infection manifesting as chronic cough.
Keywords: Organizing pneumonia; COVID-19; Post-viral syndrome; Chronic cough.
Citation: Glass LN, Hanna S, Lichtenberger JP, Milojevic I, Ahari JE. A Continuous cough after COVID-19. J Clin Images Med Case Rep. 2021; 2(3): 1158.
Introduction
Organizing pneumonia is a process of lung parenchymal injury caused by multiple etiologies. Although organizing pneumonia may be an idiopathic process, it usually occurs secondary to infection, aspiration, autoimmune disease, and post organ transplantation or radiation. Here we present a case of a chronic cough after confirmed SARS-CoV-2 (COVID-19) infection, with CT imaging consistent with organizing pneumonia. As the current COVID-19 pandemic progresses, more will be learned about long term lung sequela of this novel coronavirus. A study of Severe Acute Respiratory Syndrome-1 (SARS-CoV-1) survivors noted decreased functional status at six months compared to normal healthy individuals [1]. Delayed return to usual health among patients with a history of COVID-19 disease has been observed [2].
Case presentation
A 62-year-old man with past medical history of obstructive sleep apnea on Continuous Positive Airway Pressure therapy, chronic sinusitis, and hypothyroidism was referred to Pulmonary clinic for persistent cough of one month’s duration. Recent history was not able for a viral illness with cough, fever, and dyspnea, leading to a diagnosis of SARS-CoV-2 infection. He required one week of hospitalization and brief mechanical ventilation support. After clinical improvement, he was discharged home at the end of March 2020. His shortness of breath and fatigue improved, but his cough continued. He was seen at the end of April 2020. He was treated for a post-viral cough symptomatically with inhaled fluticasone and benzonatate. COVID antibody testing showed SARS-CoV-2 IgG was present, and PCR testing was negative. After 3 weeks of symptomatic treatment (May 2020), there was no clinical improvement. The chest radiograph was normal. He was treated for gastroesophageal reflux with a proton pump inhibitor and a course of prednisone.
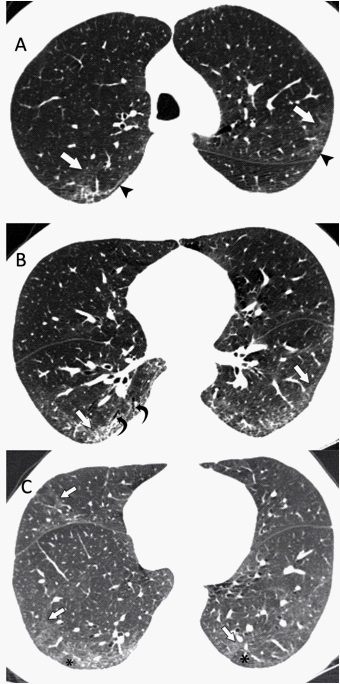
At follow-up in June 2020, pulmonary function testing results were within normal limits without obstructive or restrictive airflow limitation. His cough decreased with prednisone course (40 mg for five days), only to recur when the prednisone was stopped — A total of three prednisone courses were prescribed over a month and a half. At the end of July, after four months of chronic cough, CT imaging of the chest was performed. His SARS-CoV-2 PCR was negative and IgG antibody was positive. CT imaging showed a pattern of lung disease consistent with organizing pneumonia (Figure 1).
The differential diagnosis of chronic cough is broad. In this particular patient, common etiologies that were considered and empirically treated included post-nasal drip due to sinusitis, gastroesophageal reflux, and post-viral cough. Post viral organizing pneumonia was suspected in the setting of cough improved with prednisone. CT imaging abnormalities were critical to reaching the diagnosis of organizing pneumonia. The findings of organizing pneumonia may be subtle and mistaken for dependent atelectasis, particularly given the lower lobe predominance of COVID-19 associated lung disease. A collaborative effort between the clinician and radiologist is important to make this diagnosis.
After repeated treatment with corticosteroids, there was a significant clinical improvement. He was treated for organizing pneumonia with a prolonged course of prednisone, resulting in resolution of his symptoms.
Discussion
Organizing pneumonia is a process of lung parenchymal injury, which produces classic CT imaging findings. If no secondary cause of organizing pneumonia exists, it is considered cryptogenic organizing pneumonia. Among the secondary etiologies of organizing pneumonia are various infectious causes, including bacterial, fungal, parasitic, and viral [3]. Pathologically, organizing pneumonia indicates an injury to the alveolar epithelium with the necrosis of pneumocytes leading to granulation tissue deposited in the alveolar space [4]. The process contrasts with that of diffuse alveolar damage where there is hyaline formation in the alveoli [4]. The characteristic finding of buds of granulation tissue within the distal bronchioles, alveolar duct and alveolar sac is the histologic hallmark of organizing pneumonia [5]. Pulmonary function test may reveal mild to moderate restrictive airflow limitation depending on the extent of disease, and diffusion capacity is usually normal.
Viral infections that are known to cause organizing pneumonia include influenza, parainfluenza, herpes virus, hepatitis C, and human immunodeficiency virus [4]. A case report of Middle Eastern Respiratory Syndrome Coronavirus (MERS-CoV) infection resulted in post-viral organizing pneumonia [6]. Similar disease process after H1N1 influenza infection has also been reported [7,8]. In both cryptogenic and secondary organizing pneumonia, treatment is prolonged corticosteroid therapy.
Multiple studies have documented CT imaging consistent with organizing pneumonia associated with active COVID-19 disease. These include a review of chest CT imaging in a Brazilian hospital, where 14% of 48 patients had findings of organizing pneumonia [9]. An autopsy-based study of 7 patients with COVID-19 included one patient with organizing pneumonia on core lung biopsy [10]. A woman who presented with fever, cough, and dyspnea of 3 weeks duration, with chest CT imaging showing “Peripheral and basilar opacities with perilobular sparing” was diagnosed with COVID-19 disease based on PCR testing of bronchoalveolar lavage fluid and organizing pneumonia pathology shown on transbronchial biopsy [11]. The known association between lung infection, organizing pneumonia and possible progression to Nonspecific Interstitial Pneumonia will almost certainly impact the long-term epidemiology of COVID-19 associated pulmonary disease.
References
- Hui DS, Joynt GM, Wong KT, Gomersall CD, Li TS, et al. Impact of severe acute respiratory syndrome (SARS) on pulmonary function, functional capacity and quality of life in a cohort of survivors. Thorax. 2005; 60: 401-409.
- Tenforde MW, Kim SS, Lindsell CJ, Billig Rose E, Shapiro NI, et al. IVY Network Investigators, CDC COVID-19 Response Team, IVY Network Investigators: Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network - United States. MMWR Morb Mortal Wkly Rep. 2020; 69: 993-998.
- Baque-Juston M, Pellegrin A, Leroy S, Marquette CH, Padovani B. Organizing pneumonia: what is it?. A conceptual approach and pictorial review. Diagn Interv Imaging. 2014; 95: 771-777.
- Cordier JF, Cottin V, Lazor R, Thivolet-Béjui F. Many Faces of Bronchiolitis and Organizing Pneumonia. Semin Respir Crit Care Med. 2016; 37: 421-440.
- Couture C, Colby TV. Histopathology of bronchiolar disorders. Semin Respir Crit Care Med. 2003; 24: 489-498.
- Kim I, Lee JE, Kim KH, Lee S, Lee K, Mok JH. Successful treatment of suspected organizing pneumonia in a patient with Middle East respiratory syndrome coronavirus infection: A case report. J Thorac Dis. 2016; 8: E1190-E1194.
- Cornejo R, Llanos O, Fernández C, Carlos Díaz J, Cardemil G, et al. Organizing pneumonia in patients with severe respiratory failure due to novel A (H1N1) influenza. BMJ Case Rep. 2010; 2010: 10.
- Torrego A, Pajares V, Mola A, Lerma E, Franquet T. Influenza A (H1N1) organising pneumonia. BMJ Case Rep. 2010.
- Werberich GM, Marchiori E, Barreto MM, Rodrigues RS. Computed tomography findings in a Brazilian cohort of 48 patients with pneumonia due to coronavirus disease. Rev Soc Bras Med Trop. 2020; 53: e20200405-8682.
- Bösmüller H, Traxler S, Bitzer M, Häberle H, Raiser W, et al. The evolution of pulmonary pathology in fatal COVID-19 disease: An autopsy study with clinical correlation. Virchows Arch 2020: 1-9.
- Pogatchnik BP, Swenson KE, Sharifi H, Bedi H, Berry GJ, Guo HH. Radiology-pathology Correlation in Recovered COVID-19, Demonstrating Organizing Pneumonia. Am J Respir Crit Care Med. 2020.