
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Gouty flexor tenosynovitis – Case report and review of the literature
Hannes Prescher1*; Chad M Teven2; Deana Shenaq3; Patrick L Reavey4
1 Section of Plastic and Reconstructive Surgery, University of Chicago Medicine, Chicago, Illinois, USA.
2 Section of Plastic and Reconstructive Surgery, Mayo Clinic Phoenix, Phoenix, Arizona, USA.
3 Division of Plastic and Reconstructive Surgery, Rush Medical College, Chicago, Illinois, USA.
4 Division of Plastic and Reconstructive Surgery, University of Rochester Medical Center, Rochester, New York, USA.
*Corresponding Author: Hannes Prescher
Section of Plastic and Reconstructive Surgery, The
University of Chicago Medicine & Biological Sciences,
5841 S. Maryland Ave. Rm. J-641, MC6035, Chicago
IL, 60637, USA.
Email: hannes.prescher@uchospitals.edu
Received : Apr 19, 2021
Accepted : May 19, 2021
Published : May 21, 2021
Archived : www.jcimcr.org
Copyright : © Prescher H (2021).
Abstract
Gout is a rare cause of tenosynovitis and is difficult to diagnose based on clinical symptoms and imaging modalities. We present a case of gouty tenosynovitis of the proximal interphalangeal joint. A 32-year old male patient presented with a swollen, painful proximal interphalangeal joint of the 3rd digit on his right hand for 2 weeks with flexion contracture. Surgical exploration of the affected joint revealed a gouty tophus with extensive infiltration of the underlying flexor tendon. A tenosynovectomy and flexor tendon release was performed to treat the flexion contracture. Pathology disclosed urate crystals deposited within the tendon. Gouty infiltration of the flexor tendons of the hand can lead to extensive damage and compromised function. A high level of clinical suspicion is required as gouty tenosynovitis is a rare presentation and can often mimic an infectious etiology.
Keywords: Gout; Tenosynovitis; Flexor tendon; Hand; Tophi.
Citation: Prescher H, Teven CM, Shenaq D, Reavey PL. Gouty flexor tenosynovitis – Case report and review of the literature. J Clin Images Med Case Rep. 2021; 2(3): 1160.
Introduction
Gout is a systemic metabolic disease resulting in an inflammatory arthritis commonly seen in the first metatarsophalangeal joint, the knee, wrist and hand [1]. Clinically, gouty arthritis presents with pain, redness and swelling of the affected joint and is diagnosed by demonstration of monosodium urate crystals in the synovial fluid. Extraarticular manifestations of gout may involve bones, bursae and tendons including the flexor tendons of the hand. However, these are rare. Flexor tenosynovitis is most commonly caused by trauma or bacterial infection. The rarity of the presentation and its clinical semblance to infectious tenosynovitis therefore makes gouty tenosynovitis a unique diagnostic challenge. This can lead to misdiagnosis and a crucial delay in appropriate treatment.
Several case reports have been published in the literature describing gouty tenosynovitis affecting the flexor tendons of the hand [2-6]. Early detection of gout in distal flexor tendons of the hand is paramount as advanced disease can lead to severe damage to the flexor compartment and compromise the functional mechanism of the involved digit [7-9].
We present a case of gouty tenosynovitis with involvement of the distal flexor tendon in the hand to reinforce the diagnostic challenge of recognizing this rare presentation of gout and to emphasize the need for expeditious surgical management to prevent permanent damage to the affected flexor tendon.
Clinical case
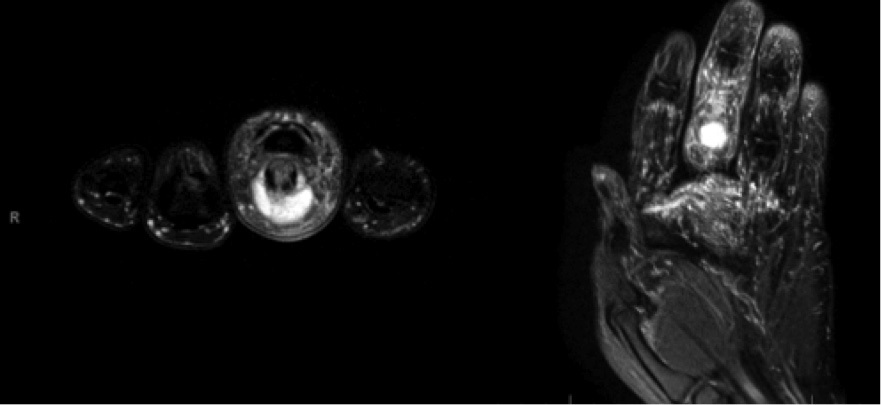
A 32-year old right-hand dominant male with a past medical history of morbid obesity and single episode of podagra presented to the emergency department with progressive swelling, pain, erythema, and loss of range of motion to his right middle finger for five days (Figure 1). There was no history of trauma. On evaluation, the finger was edematous with erythema localized to the proximal phalanx. There was a firm, nonfluctuant, and nontender mass about the volar proximal phalanx. Active and passive flexion was diminished, extension was preserved, and there was no tenderness to palpation of the flexor tendon sheath. Plain radiographs revealed soft tissue swelling without underlying fracture or malalignment. Magnetic resonance imaging demonstrated a cystic lesion (1.2 x 1.3 x 0.7 cm) on the volar aspect of the Proximal Interphalangeal (PIP) joint thought to be a ganglion cyst as well as tenosynovitis of the flexor tendon of the middle finger (Figure 2). Because the patient did not have a characteristic appearance of suppurative Flexor Tenosynovitis (FTS) but did demonstrate some concerning features, treatment with intravenous antibiotics was initiated. However, after failing to improve clinically, he was taken for operative exploration.

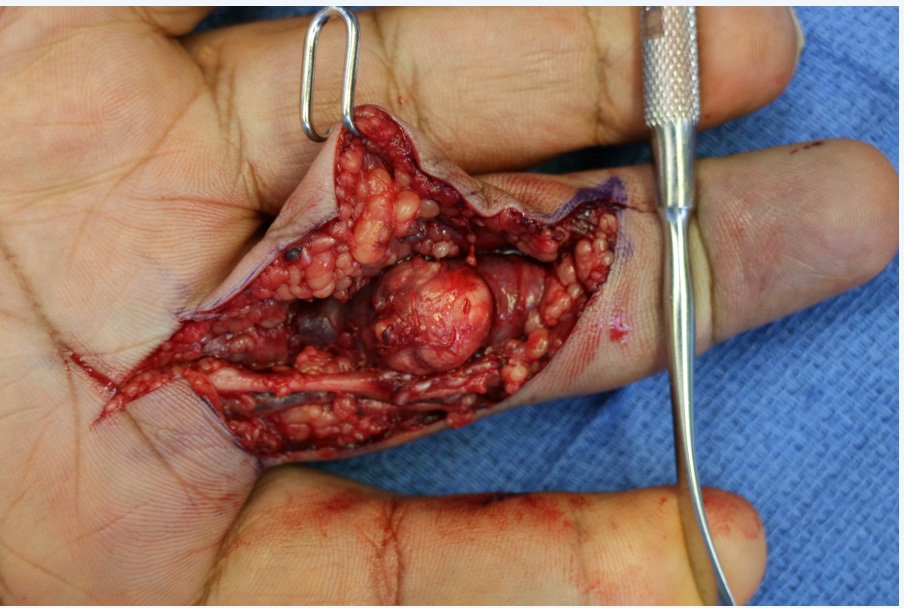
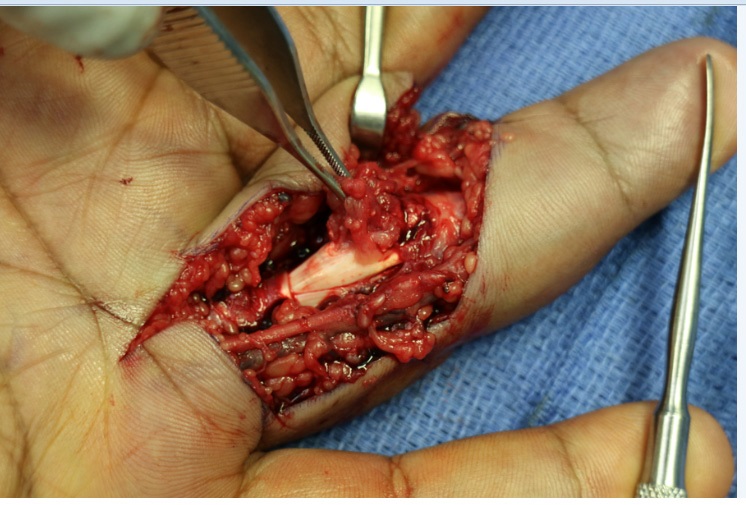
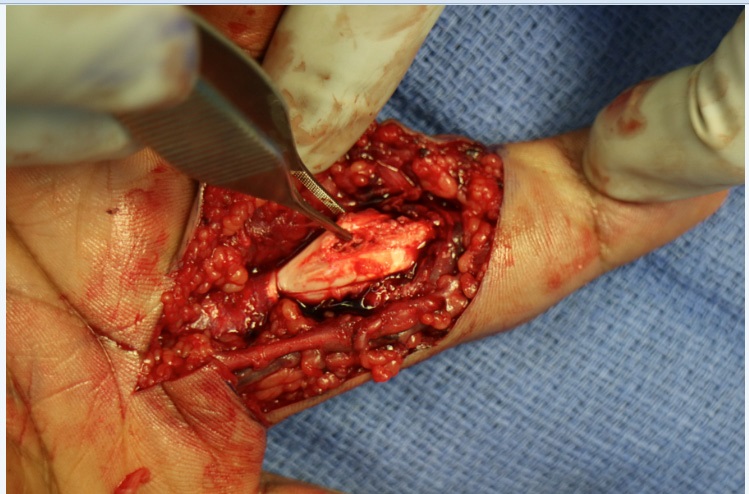
During surgery, a 1.5 x 1.5 cm mass was found emanating from the flexor tendon sheath proximal to the PIP joint and distal to the A2 pulley (Figure 3). There appeared to be cloudy fluid with crystals draining from the mass. The mass was adherent to the flexor Digitorum Profundus (FDP) tendon, which required debridement in order to fully excise the mass (Figure 4). Removal of the mass revealed significant damage to the underlying flexor tendon (Figure 5). The tendon was subsequently repaired with 5-0 proline. Additionally, there was significant tenosynovitis of the FDP and Flexor Digitorum Superficialis (FDS) tendons but no purulence or other evidence of gross infection. Passive flexion revealed palpable triggering, which improved with conservative debridement of the inflamed tendons and the A1 pulley. The wound was then irrigated and closed. Pathologic and microbiologic analysis revealed acute on chronic inflammation in the presence of gout and no evidence of infection.
Post-operatively, the patient was started on colchicine and oral steroids and discharged in good condition. At follow-up, the patient was without ongoing signs or symptoms of gout, tenosynovitis, or infection and had good function of his hand.
Discussion
Gouty infiltration of the flexor tendon sheath in the digits of the hand is uncommon but can lead to serious clinical complications. Previous case reports describe the development of carpal tunnel syndrome, as well as spontaneous tendon rupture in the upper and lower extremities in patients with gout [4,5,8,9]. Straub et al. suggest that the deposition of urate crystals within tendinous connective tissue and the subsequent inflammatory response results in collagen lysis and critical loss of connective tissue integrity, loss of tendon tensile strength and eventual rupture [10].
The proposed pathologic mechanism describes a chronic process of repeated local injury. Our patient reported only one previous episode of gout in his first metatarsophalangeal joint. Nevertheless, surgical exploration of the affected index finger revealed gouty deposits penetrating the flexor tendon sheath with severe damage to the tendon itself. The potential sequela of this disease process and the high functional acuity associated with it warrants a high index of clinical suspicion when presented with a case of flexor tenosynovitis even in a patient without an extensive history of gout.
Clinical signs of gouty flexor tenosynovitis include local warmth, pain and swelling, which can often be difficult to distinguish from infection. Magnetic resonance imaging was inconclusive in identifying a gouty tophus. In retrospect, ultrasound imaging as well as Dual-Energy CT (DECT) of the affected digit may have been of further assistance in making the diagnosis. However, we felt that the patient’s flexion contracture deformity required surgical correction and we elected to proceed with surgical exploration of the digit.
Similar to previous experiences reported in the literature, the diagnosis of gouty tenosynovitis was made upon surgical exploration. The degree of tendon damage encountered during the procedure validated our approach. Previous studies have demonstrated good clinical outcomes with surgical intervention of gouty tenosynovitis with return of complete function of the affected digit [7].
Conclusions
Gouty flexor tenosynovitis is a rare but potentially devastating clinical presentation of gout. A high index of suspicion is required to prevent misdiagnosis and delay in the initiation of treatment. Flexor tendon infiltration by monosodium urate crystal can undermine the functional integrity of the tendon leading to flexion contractures, requiring surgical intervention.
References
- Abrahamsson SO. Gouty tenosynovitis simulating an infection. A Case Report. Acta Orthop Scand. 1987; 58: 282-283.
- Aslam N, Lo S, McNab I. Gouty flexor tenosynovitis of the digits: Report of three cases. J Hand Surg Am. 2004; 29: 256.
- Hankin FM, Mayhew DE, Coapman RA, Snedden M, Schneider LH. Gouty infiltration of a flexor tendon simulating rupture. Clin Orthop. 1985; 194: 172-175.
- Hernandez-Cortes P, Caba M, Gomez-Sanchez R, Gomez-Morales M. Digital flexion contracture and severe carpal tunnel syndrome due to tophaceus infiltration of wrist flexor tendon: First manifestation of gout. Orthopedics. 2011; 34: e797-799.
- Hung JY, Wang SJ, Wu SS. Spontaneous rupture of extensor pollicis longus tendon with tophaceous gout infiltration. Arch Orthop Trauma Surg. 2005; 125: 281-284
- Moore JR, Weiland AJ. Gouty tenosynovitis in the hand. J Hand Surg. 1985; 10: 291-295.
- Primm DD Jr, Allen JR. Gouty involvement of a flexor tendon in the hand. J Hand Surg. 1983; 8: 863-865.
- Rand B, McBride TJ, Dias RG. Combined triggering at the wrist and severe carpal tunnel syndrome caused by gouty infiltration of a flexor tendon. J Hand Surg Eur. 2010; 35: 240-242.
- Schuind FA, Clermont B, Stallenberg B, Remmeling M, Pasteel JL. Gouty involvement of flexor tendons. Chir Main. 2003; 22: 46- 50.
- Straub L, Smith J, Carpenter G, Dietz G. The surgery of gout in the upper extremity. J Bone Joint Surg. 1961; 43A: 731-752.