
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Case report of isolated gastric IgG4-related lesion and series of literature review
Xiang-Xi Ye1; Tian-Hui Zou1; Juan-Tan1; Zheng Wang2; Ying-Xuan Chen1; Qin-Yan Gao1*
1 Division of Gastroenterology and Hepatology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, China.
2 Division of Surgery, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, China.
*Corresponding Author : Qin-Yan Gao
Division of Gastroenterology and Hepatology, Shanghai Institute of Digestive Disease, State Key Laboratory for Oncogenes and Related Genes, Key Laboratory of Gastroenterology & Hepatology, Ministry of
Health, Ren-Ji Hospital, Shanghai Jiao-Tong University School of Medicine, 145 Middle Shandong Road,
Shanghai, 200001, China.
Email: gaoqinyan@hotmail.com
Received : Apr 19, 2021
Accepted : May 21, 2021
Published : May 25, 2021
Archived : www.jcimcr.org
Copyright : © Gao QY (2021).
Keywords: IgG4-related disease; isolated IgG4-related gastric lesion; gastrointestinal stromal tumors.
Citation: Gao QY, Ye XX, Zou TH, Tan J, Wang Z, et al. Case report of isolated gastric IgG4-related lesion and series of literature review. J Clin Images Med Case Rep. 2021; 2(3): 1161.
Introduction
IgG4-related disease (IgG4-RD) is an immune-mediated fibroinflammatory disease that responds to glucocorticoids, which is gradually well known in recent years. It can involve multiple organs of patients, including pancreas, bile duct, gallbladder, salivary gland, orbital tissue, lung, liver, lacrimal gland, kidney, retroperitoneal, aorta, thyroid and lymph node, [1] in which gastrointestinal involvement is relatively rare [2]. Most of the known reports of isolated gastric IgG4-related lesions were accidental found (in physical examination or other site examination), and often treated as Gastrointestinal Stromal Tumors (GIST) lead to surgically resection. In addition, Calcified Fibrous Tumor (CFT) in gastrointestinal tract often occurs with submucosa [3] is histologically similar to IgG4-RD, [4] whether it belongs to IgG4-RD is still controversial.
Therefore, the diagnosis of IgG4-RD especially in GI tract remains difficult and important.
Here, we reported a case of isolated IgG4-related gastric lesion which was diagnosed as GIST and treated by surgical resection.
Case report
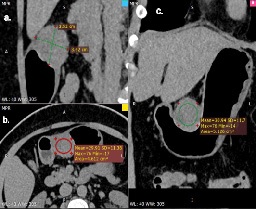
A 53-year-old woman, who was first suspected with a pancreatic mass detected on abdominal ultrasound during a routine examination, and subsequently diagnosed with GIST after detected on abdominal Computed Tomography (CT) (Figure 1) and gastrointestinal endoscopy (Figure 2), was referred to our hospital in November 2020 for further evaluation. She had a feeling of food reflux after swallowing one month before the physical examination occasionally, but presented no specific abdominal symptoms such as pain, vomiting, heartburn, dysphagia, or change in bowel habits. She had a history of hypertension which was well controlled. She also had a long-term history of eczema, allergic rhinitis, and allergic conjunctivitis, which could be relieved by taking loratadine tablets. She had no history of family history of malignant disease or autoimmune disorder.

Physical examinations were normal. The abdomen was soft and flat, and no palpable mass was observed. The laboratory results were unremarkable and the proportion of serum eosinophil was 2.3% (Reference range: 0%–5%), the total immunoglobulin level was 28.6 g/L(reference range: 20-35 g/L). Because we did not suspect IgG4-RD from preoperative studies, serum IgG4 level or other immunoglobulin were not measured.
Subsequently, the patient underwent partial gastrectomy. During the operation, the tumor was found to be located on the side of the minor curve, with a size of about 5 cm, exogenous type, and was completely resected. The pathology results showed proliferation of short spindle cells, accompanied by plenty of plasma cells and lymphocyte reactions. In order to rule out mesenchymal tumors, immunohistochemical stain were performed. The results indicated negative for CK, CD34, CD117, DOG1, S-100, SMA, ALK, and the proportion of Ki-67 is 1%. Numerous inflammatory cells stained positive for CD138 along with IgG4 with a ratio of IgG4/IgG total >40%, and a number of IgG4 positive cells >100/HPF. KIT gene exons 9, 11, 13, 17 and PDGFRA gene exons 12 and 18 were all wild type, which ruled out the possibility of GIST and finally diagnosed as IgG4- related gastric lesion. One month after the operation, the patient came to our hospital for follow-up. The surgical site was healed well, and the serum IgG4 level was 43 mg/dl. During the MRCP examination, the patient’s liver and pancreas were not found to be abnormal, and the intrahepatic and extrahepatic bile ducts were not significantly dilated or narrowed. Ultrasound examination showed no swelling of the lymph nodes or thyroid gland, and no abnormalities in the parathyroid or parotid glands.
Discussion
IgG4-RD is an immune mediated condition presenting with mass forming lesions that lead to permanent organ injury and death if left untreated [5]. Abundant IgG4 positive plasma cells in affected tissues and fibrosis represent hallmark pathological features of this disorder. Definitive diagnosis of IgG4-RD requires rigorous clinical-pathological correlation because clinical assessments, laboratory evaluations, and imaging studies are often insufficient to distinguish neoplastic, inflammatory, and infections [6].
The comprehensive diagnostic criteria for IgG4-RD are divided into three categories: 1) diffuse or localized swelling or masses in single or multiple organs; 2) elevated serum IgG4 concentrations >135 mg/dL, and 3) histopathological findings including marked lymphocyte and plasmacytic infiltration and fibrosis, infiltration of IgG4-positive plasma cells in a ratio of IgG4-positive plasma cells/IgG-positive plasma cell >40%, and >10 IgG4-positive plasma cells/HPF. Histopathological features of IgG4-RD including: 1) Dense lymphocytic infiltration; 2) Storiform fibrosis (spindle-shaped fibroblasts or myofibroblasts aligned in a pattern resembling bicycle wheel spokes); 3) Obliterative phlebitis (vessels filled with lymphocyte and plasma cell infiltration) [1,6].
Although IgG4-RD has relatively clear diagnostic criteria, there is no clear and complete diagnostic criteria and process for IgG4-related gastric lesions. There are doubts about whether IgG4-related gastrointestinal diseases belongs to IgG4-RD, which needs to be studied [2]. Among the 17 cases in previous reports, 15 cases (88.2%) were misdiagnosed as GIST (see Table 1), which indicated the extremely confusion between GIST and IgG4-related gastric lesions.
Table 1: Isolated gastric IgG4-related lesion.
No. |
Study |
Sex |
Age |
Symptom |
Diagnosis |
Location |
Size(cm) |
IgG4 levels |
Time |
CD34 |
treatment |
1 |
Rollins et al.20111 |
F |
75 |
asymptom |
GIST |
body |
5.6×5.0 |
Normal |
Postoperative |
+ |
SR |
2 |
Kim et al. 20122 |
F |
59 |
asymptom |
GIST |
—— |
3.3×1.4 |
Normal |
Postoperative |
—— |
SR |
3 |
Kim et al. 20122 |
F |
56 |
asymptom |
GIST |
—— |
2.1×1.5 |
Normal |
Postoperative |
—— |
SR |
4 |
Na et al. 20123 |
M |
56 |
anorexia, nausea and abdominal |
nodule |
Body |
0.8 |
—— |
—— |
—— |
ER |
5 |
Bulanov et al. 20164 |
F |
62 |
asymptom |
gastric cancer |
Antrum |
8.0×3.0 |
Elevated |
Postoperative |
—— |
SR |
6 |
Cheong et al. 20165 |
F |
27 |
asymptom |
GIST/NET |
fundus |
3.4×1.6 |
Normal |
Postoperative |
- |
SR |
7 |
Otsuka et al. 20166 |
M |
44 |
abnormalities on an upper gastrointestinal |
GIST |
Body |
2.0×1.8 |
Normal |
Postoperative |
—— |
ESD |
8 |
Woo et al. 20167 |
F |
48 |
vomiting, |
GIST/NET |
Body |
3.6×2.2 |
Normal |
Postoperative |
+ |
SR |
9 |
Bohlok et al. 20188 |
M |
57 |
asymptom |
GIST |
antral |
1.7×1.6 |
Normal |
Postoperative |
- |
SR |
10 |
Seo et al. 20189 |
F |
40 |
asymptom |
GIST |
angle |
4.3×2.7 |
Normal |
Postoperative |
- |
SR |
11 |
Seo et al. 20189 |
F |
44 |
asymptom |
GIST |
fundus |
4.1×3.0 |
—— |
—— |
- |
SR |
12 |
Skorus et al. 201810 |
F |
29 |
asymptom |
GIST |
Body |
2.0×1.5 |
—— |
—— |
—— |
SR |
13 |
Cho et al. 202011 |
M |
45 |
asymptom |
GIST |
Body |
3.0×2.8 |
—— |
—— |
—— |
SR |
14 |
Ramakrishna et al. 202012 |
M |
43 |
asymptom |
GIST |
Antrum |
7.0×5.0 |
Elevated |
Postoperative |
—— |
SR |
15 |
Ramakrishna et al. 202012 |
M |
58 |
erosive |
GIST |
Body |
4.5×4.0 |
Elevated |
Postoperative |
—— |
SR |
16 |
Yamane et al. 202013 |
F |
70 |
asymptom |
GIST |
Body |
1.5 |
Elevated |
Preoperative |
—— |
SR |
17 |
presented case. 2021 |
F |
53 |
feeling of food reflux after |
GIST |
Body |
3.5×3.5 |
Normal |
Postoperative |
- |
SR |
F: Female, M: Male; Time: Time to measure serum IgG4 level; SR: Surgical Resection; ER: Endoscopic Resection; ESD: Endoscopic Submucosal Dissection 1. Rollins K, Mehta S, O'Donovan M, et al. Gastric IgG4-Related Autoimmune Fibrosclerosing Pseudotumour: A Novel Location. ISRN Gastroenterol. 2011; 2011: 873087. 2. Kim D, Kim J, Park D, et al. Immunoglobulin G4-related inflammatory pseudotumor of the stomach. Gastrointest Endosc. 2012; 76: 451-452. 3. Na K, Sung J, Jang J, et al. Gastric nodular lesion caused by IgG4-related disease. Pathol Int. 2012; 62: 716-718. 4. Bulanov D, Arabadzhieva E, Bonev S, et al. A rare case of IgG4-related disease: a gastric mass, associated with regional lymphadenopathy. BMC Surg. 2016; 16: 37. 5. Cheong H, Lee B, Song G, et al. Immunoglobulin G4-Related Inflammatory Pseudotumor Presenting as a Solitary Mass in the Stomach. Clin Endosc. 2016; 49: 197-201. 6. Otsuka R, Kano M, Hayashi H, et al. Probable IgG4-related sclerosing disease presenting as a gastric submucosal tumor with an intense tracer uptake on PET/CT: A case report. Surg Case Rep. 2016; 2: 33. 7. Woo C, Yook J, Kim A, et al. IgG4-Related Disease Presented as a Mural Mass in the Stomach. J Pathol Transl Med. 2016; 50: 67-70. 8. Bohlok A, Khoury M, Tulelli B, et al. A rare presentation of IgG4 related disease as a gastric antral lesion: Case report and review of the literature. Int J Surg Case Rep. 2018; 51: 244-247. 9. Seo H, Jung Y, Park C, et al. IgG4-related Disease in the Stomach which Was Confused with Gastrointestinal Stromal Tumor (GIST): Two Case Reports and Review of the Literature. J Gastric Cancer. 2018; 18: 99-107. 10. Skorus U, Kenig J, Mastalerz K. IgG4-related disease manifesting as an isolated gastric lesion- a literature review. Polski przeglad chirurgiczny. 2018; 90: 41-45. 11. Cho M, Moon H, Lee H, et al. Immunoglobulin G4-related disease in the stomach presenting as a gastric subepithelial tumor: Case report. Medicine. 2020; 99: e22078. 12. Ramakrishna B, Yewale R, Vijayakumar K, et al. Gastric IgG4-related disease presenting as a mass lesion and masquerading as a gastrointestinal stromal tumor. J Pathol Transl Med. 2020; 54: 258-262. 13. Yamane T, Eto K, Morinaga T, et al. IgG4-related disease presenting as a submucosal tumor of the stomach resected with laparoscopic endoscopic cooperative surgery: a case report. Surg Case Rep. 2020;6:93.
Among the 17 IgG4-related gastric lesions cases , 64.7% were female, most of which were middle-aged (median age of 53), while the median age of onset of GIST is 65 years old, which seems to be older than that of IgG4-related gastric lesions. In addition, GISTs may occur in children, which has not been reported in cases of isolated IgG4-related gastric lesions. There is no significant gender difference in the incidence of GIST [7], while a disposition to female in IgG4-related gastric lesions were found.
Except for a small number of patients who may have some non-specific symptoms and signs before and after detection, most IgG4-related gastric lesions patients were found asymptom. However, GISTs may bleeding into the abdominal cavity or bowel which is a common presentation. Bleeding may be slow, resulting in anemia, or sudden, causing tachycardia, fainting, stomach pain, melena, or hematemesis. Also, GISTs may cause other symptoms depending on size and location, such as abdominal pain, fullness or pressure, or bowel obstruction. In addition, malignant GISTs often has abdominal and liver metastases [7,8]. But unfortunately, none of the symptoms and signs can help to differentiated GIST with isolated IgG4-related gastric lesions before operation.
IgG4-related gastric lesions may involve all part of the stomach, mostly in the body of the stomach. The size of the lesions was more than 1 cm, and most of them were more than 3 cm. Although GISTs could occur in anywhere along the gastrointestinal tract, the most common place is stomach (50–60%) [9]. In a retrospective study of 187 patients with gastric stromal tumors, according to tumor site in the stomach: 69 (36.9%) in the upper third; 103 (55.1%) in the middle third; and 15 (8.0%) in the lower third. The median tumor sizes in the upper, middle, and lower third were 9.21 cm, 7.5 cm, and 3.92 cm, respectively [10].
In terms of imaging of these two kinds of diseases, there was no significant difference in CT, endoscope, or endoscopic ultrasonography. Most of them showed as soft tissue with density mass, clear boundary, regular shape, and no adhesion with the surrounding [8]. In some studies, PET/CT has a certain value in diagnosis, which shows an intense tracer uptake by the tumor in the upper part of the stomach [11]. Generally speaking, metastasis of GISTs may occur when CT shows tumor > 5 cm, lobulation, inhomogeneous enhancement, mesenteric fat infiltration, ulcer, regional lymph node enlargement or exogenous growth [12], but there are no reports about the metastasis of IgG4-related gastric lesion.
The level of serum IgG4 may be elevated or normal. Among the 17 cases, only one case had the elevated serum IgG4 level. Unfortunately, the serum IgG4 level was not measured before surgery in our case. However, measurement of serum IgG4 is not free from analytical errors. Most laboratories worldwide quantify IgG4 concentration by either turbidimetry or nephelometry, with the former method giving spuriously normal IgG4 values in case of antigen excess (“prozone phenomenon”) [13].
From this, it appears that histology and immunohistochemistry are very important. Most GISTs demonstrate three main histologic subtypes: spindle cell type (most common), epithelioid type, and mixed spindle and epithelioid type, among them, spindle cell GIST may be similar to isolated IgG4-related gastric lesions, which composed of cells arranged in short fascicles and whorls. Many gastric spindle cell GISTs show extensive paranuclear vacuolization [7,14]. Confusions may occur when the characteristic histological features of IgG4-RD are not observed. The disease was clearly differentiated from GIST at the pathological and immunohistochemical level. Generally speaking, when GIST staining, CD117 (KIT), CD34 and DOG1 are likely to be positive, and GIST may have mutations in exons 9, 11, 13, 17 of KIT gene and exons 12 and 18 of PDGFRA gene. When staining tissues of IgG4-related gastric lesions, CD34 might be positive, CD138 on behalf of plasma cells is positive, and other highly suggestive markers of GIST are negative, which can clearly distinguish the two. It was reported in previous reports that the lesion is pseudotumor because it was an inflammatory lesion [15], and IgG4‐related gastrointestinal diseases were classified into two types: One is a gastrointestinal lesion showing marked thickening of the wall, and the other is an IgG4-related pseudotumor [2]. Regrettably, although some lesions were punctured with insufficient depth, the corresponding immunohistochemical staining was not performed. More identification methods need to be discovered and applied.
The general first-line treatment of IgG4-RD is still low-dose glucocorticoid [16], while the second line is mainly DMARDs (AZA-MTX-CTX-MMF-LFN-CSA), and the third-line drug is biological agent (rituximab). However, because there are few cases of IgG4-RD involving the digestive tract independently, there is no clear guidance on the treatment of this in the literature [6]. Treatment of GIST is completely different, approximately 60% of patients with localized GIST are cured with surgery. Imatinib is used before surgery and as an adjuvant [7].
It is worth noting that, gastric calcifying fibrous tumor (CFT) and IgG4-related gastric lesions are also difficult to distinguish. There are two completely different treatments for the two diseases. Calcifying fibrous tumor (CFT) is a rare mesenchymal lesion, and it may occur at virtually any age, with a predilection for adults and for females. They occur most commonly in the stomach and the small and large intestines. CFTs are most often found incidentally, cured by local resection, and have a low risk of recurrence. Histology shows three characteristic features: Spindle cell proliferations within a densely hyalinized stroma, scattered calcifications, and lymphoplasmacytic inflammation. CFTs are immunoreactive for CD34, vimentin and factor XIIIa, helping to distinguish them from other benign mesenchymal neoplasms. The plasma cells in CFT may stain positively for IgG and IgG4, which has raised the possibility that CFT may be a manifestation of IgG4-related disease (IgG4-RD) [17]. Similar to CFT, IgG4-RD gives rise to inflammatory mass lesions that are clinically benign. Among the reported cases of CFT, obliterative phlebitis was not identified in all those cases, and the serum IgG4 levels were not elevated, which may help to distinguish.
IgG4-related gastric lesions should also be distinguished from Leiomyomas, gastrointestinal schwannoma. Immunohistochemistry in leiomyomas shows positivity for SMA and desmin [18]; gastrointestinal schwannomas, definitive exclusion of schwannoma is best accomplished by S100 staining, which is diffusely positive in schwannoma and negative in our case [19].
Conclusion
IgG4-related gastric lesions that lack of diagnostic methods other than pathology and immunohistochemistry appear to be difficult to diagnose. It is of utmost importance to rule out other gastrointestinal submucosal masses such as GIST, which determines a completely different treatment. To avoid unnecessary resection, IgG4-related gastric lesions should be considered in the differential diagnosis, and be taken in consideration when similar cases appear.
References
- Stone J, Zen Y, Deshpande V. IgG4-related disease. The New England journal of medicine 2012; 366: 539-551.
- Koizumi S, Kamisawa T, Kuruma S, et al. Immunoglobulin G4- related gastrointestinal diseases, are they immunoglobulin G4- related diseases? World journal of gastroenterology. 2013; 19: 5769-5774.
- Zhang H, Jin Z, Ding S. Gastric calcifying fibrous tumor: A case of suspected immunoglobulin G4-related gastric disease. Saudi journal of gastroenterology: official journal of the Saudi Gastroenterology Association. 2015; 21: 423-426.
- Turbiville D, Zhang X. Calcifying fibrous tumor of the gastrointestinal tract: A clinicopathologic review and update. World journal of gastroenterology. 2020; 26: 5597-5605.
- Patel N, Anzalone M, Buja L, et al. Sudden cardiac death due to coronary artery involvement by IgG4-related disease: a rare, serious complication of a rare disease. Archives of pathology & laboratory medicine. 2014; 138: 833-836.
- Lanzillotta M, Mancuso G, Della-Torre E. Advances in the diagnosis and management of IgG4 related disease. BMJ (Clinical research ed). 2020; 369: m1067.
- von Mehren M, Joensuu H. Gastrointestinal Stromal Tumors. Journal of clinical oncology: Official journal of the American Society of Clinical Oncology. 2018; 36: 136-143.
- Zhang L, Smyrk T, Young W, et al. Gastric stromal tumors in Carney triad are different clinically, pathologically, and behaviorally from sporadic gastric gastrointestinal stromal tumors: findings in 104 cases. The American journal of surgical pathology. 2010; 34: 53-64.
- Joensuu H, Hohenberger P, Corless C. Gastrointestinal stromal tumour. Lancet (London, England). 2013; 382: 973-983.
- Huang H, Liu Y, Zhan Z, et al. Different sites and prognoses of gastrointestinal stromal tumors of the stomach: report of 187 cases. World journal of surgery. 2010; 34: 1523-1533.
- Otsuka R, Kano M, Hayashi H, et al. Probable IgG4-related sclerosing disease presenting as a gastric submucosal tumor with an intense tracer uptake on PET/CT: A case report. Surgical case reports. 2016; 2: 33.
- Burkill G, Badran M, Al-Muderis O, et al. Malignant gastrointestinal stromal tumor: distribution, imaging features, and pattern of metastatic spread. Radiology. 2003; 226: 527-532.
- Khosroshahi A, Cheryk L, Carruthers M, et al. Brief Report: Spuriously low serum IgG4 concentrations caused by the prozone phenomenon in patients with IgG4-related disease. Arthritis & rheumatology (Hoboken, NJ). 2014; 66: 213-217.
- Patil D, Rubin B. Gastrointestinal stromal tumor: Advances in diagnosis and management. Archives of pathology & laboratory medicine 2011; 135: 1298-1310.
- Kim D, Kim J, Park D, et al. Immunoglobulin G4-related inflammatory pseudotumor of the stomach. Gastrointestinal endoscopy. 2012; 76: 451-452.
- Khosroshahi A, Wallace Z, Crowe J, et al. International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease. Arthritis & rheumatology (Hoboken, NJ). 2015; 67: 1688-1699.
- Miettinen M, Sarlomo-Rikala M, Sobin L, et al. Esophageal stromal tumors: A clinicopathologic, immunohistochemical, and molecular genetic study of 17 cases and comparison with esophageal leiomyomas and leiomyosarcomas. The American journal of surgical pathology. 2000; 24: 211-222.
- Voltaggio L, Murray R, Lasota J, et al. Gastric schwannoma: A clinicopathologic study of 51 cases and critical review of the literature. Human pathology. 2012; 43: 650-659.